If your front-end staff dreads Monday mornings because the PA queue has exploded over the weekend, you’re not alone. Prior authorization bottlenecks are quietly draining provider revenue, delaying patient care, and burning out your best staff. In this guide, you’ll get a clear, practical roadmap to identify where your process is breaking down and exactly what to do to fix it.
93% of physicians say PA delays necessary care
39 PA requests per physician per week on average
$31B estimated annual revenue lost to PA inefficiencies
13 hrs spent weekly per physician on PA paperwork
Why Prior Authorization Bottlenecks Are Getting Worse
Prior authorization isn’t a new concept, but the administrative weight of managing it keeps growing. In 2024 alone, Medicare Advantage insurers processed nearly 53 million PA requests, denying approximately 4.1 million of them. That’s a 7.7% denial rate that hits directly at patient access and practice cash flow.
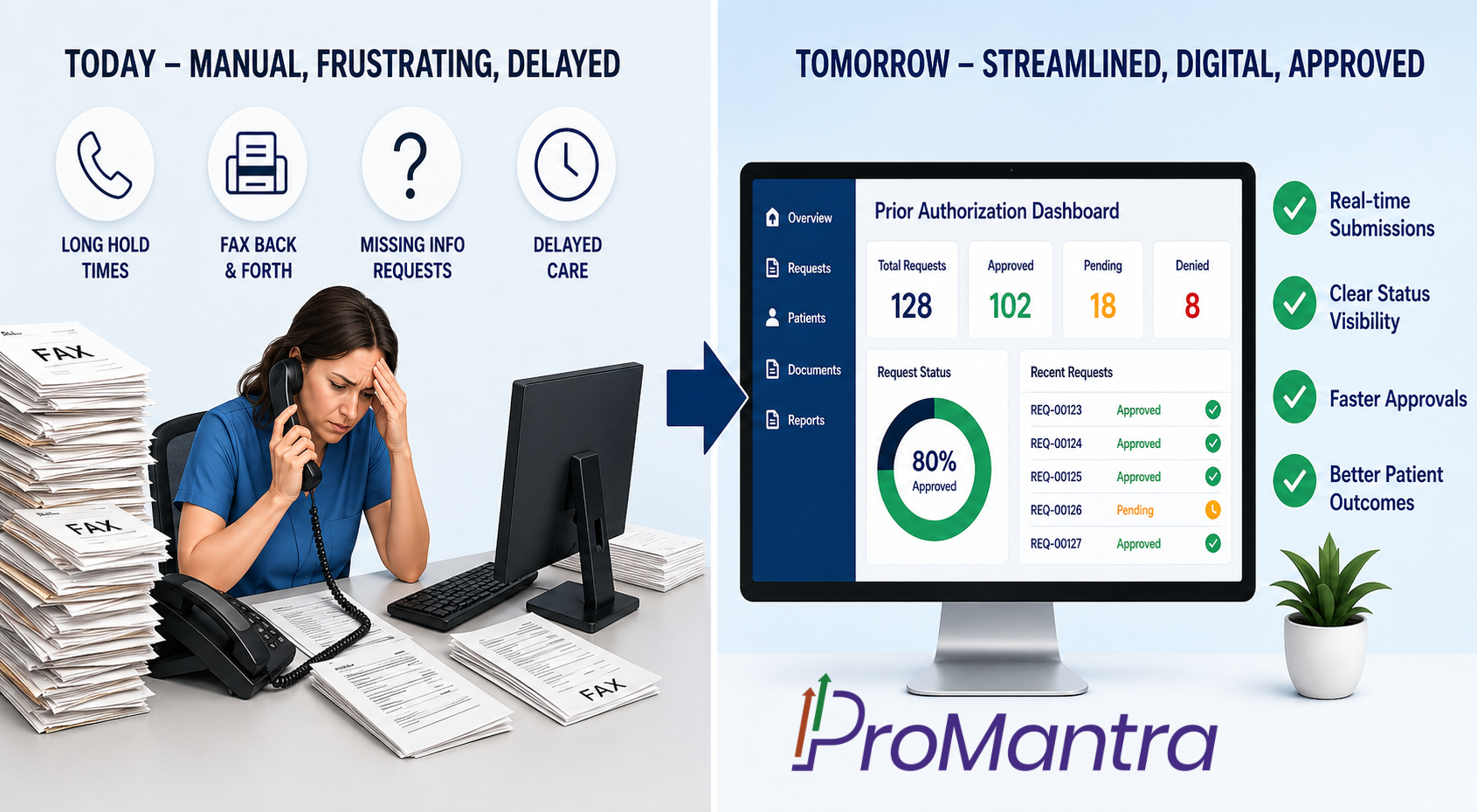
The problem isn’t just volume. It’s the manual, disconnected, and error-prone nature of how most practices handle PA today. Phone calls to insurance reps, fax-based submissions, payer portals that change without notice, and unclear documentation requirements, it all adds up to a process that’s broken by design.
“82% of clinicians report that patients abandon treatment due to prior authorization complexity.” AMA Prior Authorization Survey, 2024
When patients walk away from care they need because of administrative friction, that’s not just a revenue problem. It’s a patient safety crisis. According to the AMA’s 2024 survey, 29% of physicians have seen a life-threatening or serious adverse event tied directly to a PA delay.
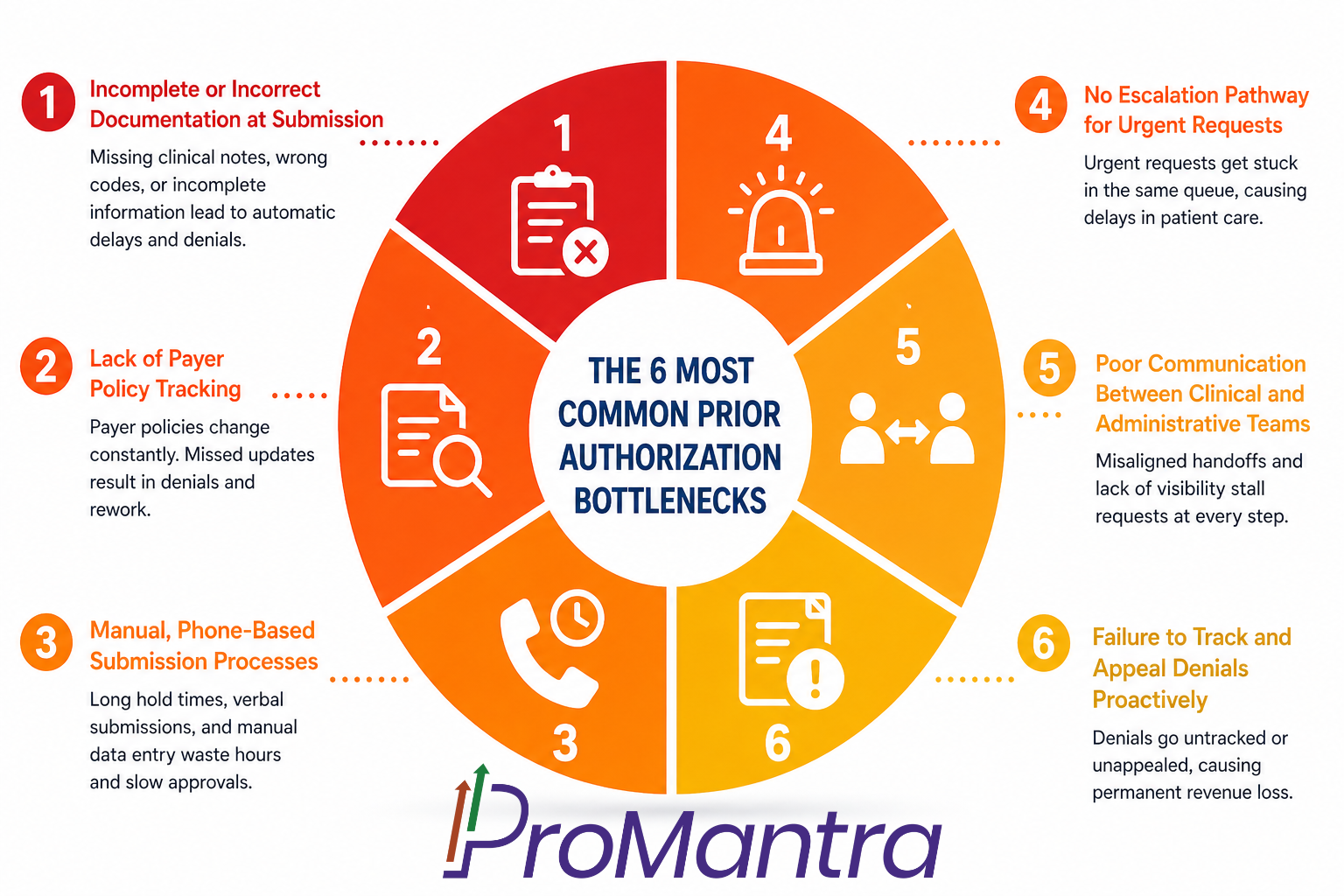
The 6 Most Common Prior Authorization Bottlenecks
Before you can fix the problem, you need to know exactly where the process is choking. Here are the six prior authorization bottlenecks that consistently show up across practices of every size:
1. Incomplete or Incorrect Documentation at Submission
This is the number-one culprit. According to Experian’s 2024 State of Claims report, 46% of claim denials are caused by missing or inaccurate information at submission like wrong diagnosis codes, absent clinical notes, or mismatched procedure codes.
Every incomplete submission means a payer can legitimately reject or delay the request, and your staff has to start over. One bad submission can set a case back by 5 to 10 business days.
2. Lack of Payer Policy Tracking
Payer policies change constantly and they rarely send your practice a memo. A mid-sized Texas clinic discovered this the hard way when their payer updated MRI approval criteria to require proof that physical therapy had failed first. Because the clinic missed the update, 35% of their MRI requests were denied in Q1 alone, according to Practolytics case research (2025).
If your team isn’t proactively monitoring payer bulletins and LCD/NCD updates, you’re flying blind.
3. Manual, Phone-Based Submission Processes
Phone-based PA submission is one of the biggest time sinks in any practice. The average medical practice spends roughly 13 staff hours per physician per week on prior authorization-related tasks. Most of that time goes into hold queues, verbal back-and-forths, and manual data entry after the call.
4. No Escalation Pathway for Urgent Requests
Urgent PA requests need their own workflow lane. CMS now requires payers to return decisions within 72 hours for urgent requests and 7 calendar days for standard ones. But if your practice treats urgent and routine requests the same way, approvals slip and patients wait.
5. Poor Communication Between Clinical and Administrative Teams
The PA process sits at the intersection of clinical care and billing. When those two teams aren’t aligned when the clinician orders a procedure without flagging it for PA, or the admin team doesn’t loop in the physician for peer-to-peer review requests, stall at every handoff.
6. Failure to Track and Appeal Denials Proactively
Most practices accept an initial denial as final. They shouldn’t. The majority of PA denials are overturnable on appeal when the right supporting documentation is submitted. However, without a structured denial tracking and appeals workflow, those dollars simply disappear.
Quick Check: How many of these six bottlenecks exist in your current PA workflow? If you’re counting more than two, you’re likely losing significant revenue and clinical capacity every single week.
A Practical Roadmap to Fix Prior Authorization Bottlenecks
Here’s what actually works. Use this as your phased improvement roadmap whether you’re a small practice or a multi-specialty group.
1 Audit Your Current PA Denial Rate by Payer and CPT Code
Start with the data. Pull a 90-day report on PA-related denials broken down by payer, service type, and reason code. You’ll almost always find that 20% of your payers are responsible for 80% of your denials and fixing those relationships drives the most immediate ROI.
2 Build Payer-Specific PA Checklists
Create a checklist for every major payer that covers required diagnosis codes, clinical criteria, documentation attachments, and submission format preferences. A one-page reference sheet for the 10 payers that generate most of your PA volume can cut submission errors dramatically.
3 Designate a PA Specialist or Team
Centralizing PA responsibilities under a dedicated specialist rather than spreading it across your general billing team dramatically reduces error rates. This person owns payer policy monitoring, submission quality, and denial escalation. Even in small practices, carving out this role pays for itself fast.
4 Implement Electronic PA (ePA) Submissions Wherever Possible
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) now requires payers to support FHIR-based PA APIs. By 2027, 80% of electronic PA requests with proper documentation should be answered in real-time. Start integrating ePA capabilities into your EHR workflow now, don’t wait for the deadline to catch you unprepared.
5 Create a Denial Management and Appeals Protocol
Track every PA denial in a dedicated log. Categorize by reason code. Assign a response timeline. For clinical denials, schedule peer-to-peer review requests immediately most payers grant these within 48 to 72 hours. A structured appeals process typically recovers 40–60% of initially denied PAs. Read more about Prior Authorization delays in our blog here.
6 Monitor Gold Carding Opportunities
As of 2026, five states have enacted gold carding programs which are Texas, Louisiana, Michigan, Vermont, and West Virginia. If your practice has a 90%+ approval rate on specific service lines, you may already qualify for exemption. Track your approval history by CPT code and payer to identify where you can seek gold card status and reduce your overall PA volume.
What’s Changing: Regulatory Tailwinds You Should Know
If you’ve felt like the system is working against you on PA, the regulatory landscape is finally shifting in your favor though only if you’re prepared to take advantage of it.
CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)
Effective across Medicare Advantage, Medicaid, CHIP, and ACA marketplace plans, this rule mandates that payers issue decisions within 7 calendar days for standard requests and 72 hours for urgent ones. Payers must also provide clear written reasons for denials, no more vague rejections that leave your team guessing.
Starting in 2027, 80% of electronic PA requests with required documentation must be answered in real time. That’s a significant operational shift that practices need to plan for today.
Industry-Wide Voluntary Commitments for 2026
In June 2025, major health insurers voluntarily pledged to reduce the volume of services requiring PA, honor PA approvals during coverage transitions, and move toward real-time approvals on most requests by 2027. While voluntary doesn’t mean guaranteed, the direction of travel is clear.
State-Level PA Reform Legislation
At least 18 states took legislative action on PA in 2025 alone. If you practice in a state with active PA reform legislation, your compliance team needs to be tracking those timelines. Some state rules go beyond CMS mandates and apply to commercial payers not covered by federal rule.
💡 ProMantra Insight: At ProMantra, we actively monitor CMS and state-level PA policy changes on behalf of our clients. Our Revenue Cycle Management teams update submission protocols in real time, so your practice is always aligned with the current rules, not the ones from last quarter. Learn how our prior authorization services reduce your denial rate from day one.
How a Revenue Cycle Management Partner Can Solve This for You
Managing prior authorization bottlenecks in-house is possible, but it’s resource-intensive. As PA volume grows and payer requirements multiply, most practices find that a dedicated RCM partner delivers faster results at lower operational cost.
Here’s what a strong RCM partner brings to your PA process:
- Real-time payer policy monitoring so your submissions are always aligned with current criteria
- Dedicated PA specialists who handle submission, follow-up, and denial escalation end to end
- Technology-enabled workflows that reduce manual steps and track approval timelines automatically
- Denial analytics and reporting so you can see exactly where approvals are failing and why
- Appeals management to recover revenue from initial denials that should have been approved
At ProMantra, our end-to-end Revenue Cycle Management services are specifically designed to take the administrative burden of prior authorization off your clinical staff’s plate, so your team can focus on care, not paperwork. From eligibility verification to peer-to-peer coordination, we manage the full PA lifecycle on your behalf.
Frequently Asked Questions
What are the most common reasons prior authorization requests get denied?
The most frequent denial reasons include missing or incomplete clinical documentation, incorrect diagnosis or procedure codes, failure to meet payer-specific medical necessity criteria, and submission to the wrong insurance division. According to Experian’s 2024 State of Claims report, 46% of claim denials trace back to missing or inaccurate information all of which is preventable with the right pre-submission checklist and trained staff.
How long does a prior authorization typically take to get approved?
Under the new CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), payers are now required to respond within 7 calendar days for standard requests and 72 hours for urgent ones. However, manual submissions via phone or fax can still take significantly longer, often 7 to 14 business days due to incomplete documentation or payer processing backlogs. Electronic PA submissions through FHIR-based APIs are the fastest path to approval.
Can a prior authorization denial be appealed, and is it worth the effort?
Absolutely. Most PA denials, especially those categorized as “not medically necessary”are overturnable on appeal when supporting clinical documentation is provided. Practices with structured denial management workflows typically recover 40–60% of initially denied PAs. Peer-to-peer reviews with the payer’s medical director are particularly effective for complex clinical cases. If your practice isn’t routinely appealing PA denials, you’re leaving significant revenue on the table.
What is “gold carding” in prior authorization, and how can my practice qualify?
Gold carding is a program that exempts physicians with a strong PA approval track record from having to seek prior authorization for specific services. To qualify in most states, a provider typically needs to have submitted at least five PA requests for a specific service with a 90% or higher approval rate. As of 2026, gold carding is available in Texas, Louisiana, Michigan, Vermont, and West Virginia, with more states actively considering similar legislation. Tracking your PA approval rate by CPT code is the first step to identifying gold card eligibility.
Stop Letting Prior Authorization Bottlenecks Drain Your Revenue
ProMantra’s Revenue Cycle Management experts handle your entire prior authorization workflow from first submission to final approval. Contact Us to request a free RCM consultation.