When CMS announced the 2026 Medicare Physician Fee Schedule, the headline number was encouraging. For the first time in years, Congress passed a 2.5% positive update to the conversion factor, giving providers a brief moment of relief after a long stretch of annual cuts.
But here is the part that did not make many headlines.
That same final rule also introduced a new 2.5% efficiency adjustment on work RVUs for non-time-based services, along with a significant site-of-service payment differential that cuts indirect practice expense reimbursements for facility-based services by roughly 50%. For many providers, especially those who perform procedures in hospital or outpatient facility settings, the net impact of the 2026 Medicare fee schedule is not an increase. It is a reduction.
According to the American Medical Association, 81% of infectious disease physicians face cuts of 5% or more under the new rule. Orthopedic surgery faces an overall impact of roughly negative 5% when efficiency adjustments are factored in. Cardiology services performed in a facility setting are projected to decline 7%.
If your practice has not gone line by line through your 2026 reimbursements and compared them against what you should be receiving, you may already be leaving money on the table right now.
In this blog, you will get a plain-language breakdown of the key 2026 Medicare fee schedule changes, a step-by-step reimbursement audit process, and a practical checklist your billing team can use starting today.
What Actually Changed in the 2026 Medicare Fee Schedule
Before you can audit your reimbursements, you need to understand what changed and why it matters.
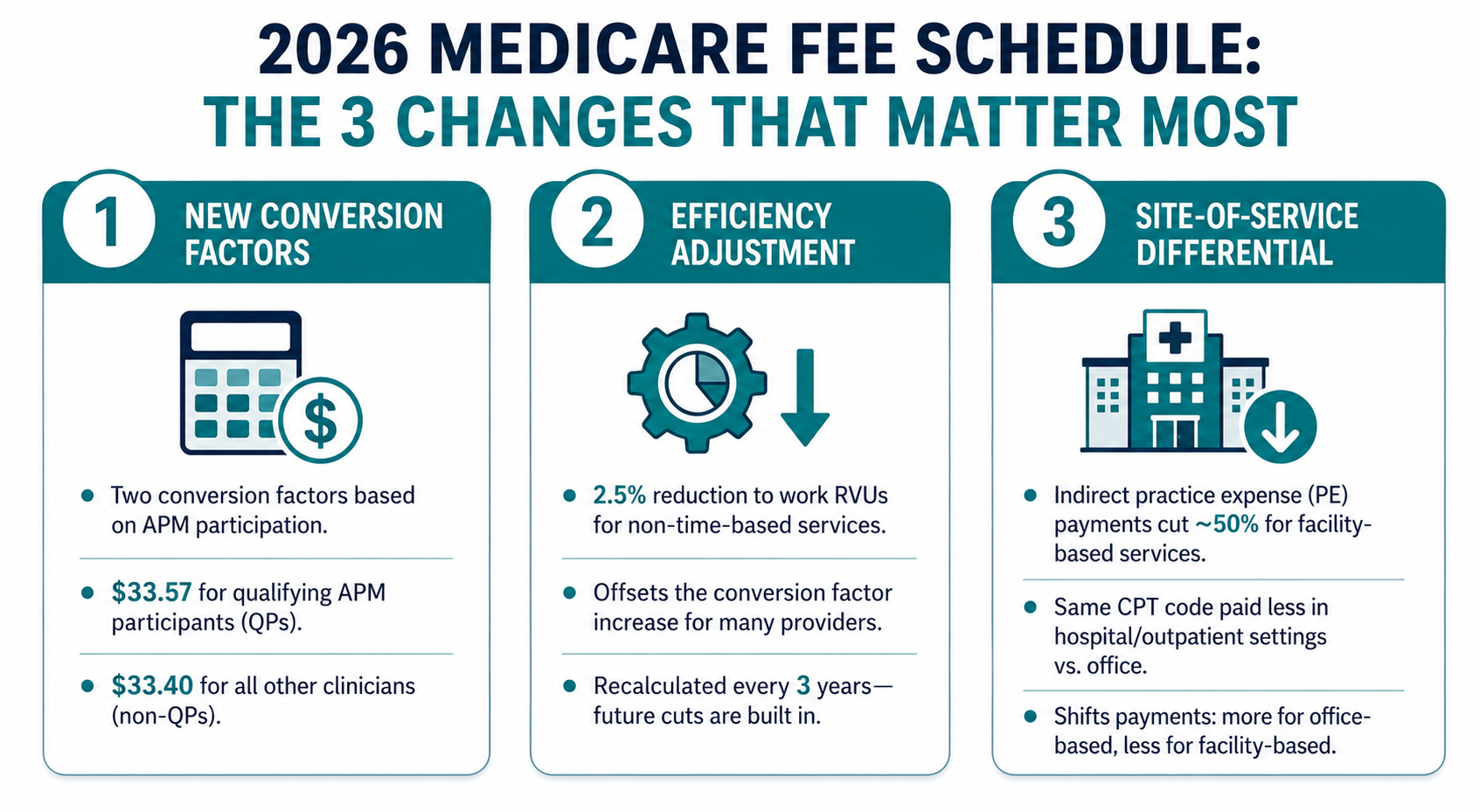
Change 1: Two Separate Conversion Factors
For the first time ever, the 2026 Medicare Physician Fee Schedule established two distinct conversion factors based on Alternative Payment Model (APM) participation.
According to the CMS final rule and confirmed by the American Society of Hematology’s detailed rule summary:
- Qualifying APM participants (QPs): conversion factor of $33.57, an increase of approximately 3.77% from the 2025 rate of $32.35
- All other clinicians (non-QPs): conversion factor of $33.40, an increase of approximately 3.62%
These are the baseline rates used to calculate Medicare reimbursement. Every service payment flows through one of these two numbers. If your practice participates in a qualifying APM, your conversion factor is modestly higher. If not, you are on the lower track.
The practical takeaway: check which conversion factor applies to your practice and make sure your billing system reflects the correct rate. Using the wrong conversion factor in your payment calculations will cause you to either miss underpayments or fail to appeal accurately.
Change 2: The 2.5% Efficiency Adjustment on Work RVUs
This is the change that is quietly canceling out the conversion factor increase for a large number of practices.
CMS finalized a 2.5% reduction to work RVUs for non-time-based services. The agency argues that physician surveys used to determine work values may overstate the effort involved, particularly for procedural services that have become more efficient due to technology improvements.
The result, as Spry’s 2026 RVU analysis points out, is that while conversion factors increased by roughly 3.6% to 3.8%, the efficiency adjustment reduces overall specialty payments by approximately 1% for most procedural specialties. That effectively neutralizes the headline increase for many providers.
It gets worse for high-volume procedural specialties. Orthopedic surgery, interventional radiology, neurosurgery, and other procedural-heavy fields face disproportionate exposure because the adjustment applies across the bulk of their billed service volume. And this is not a one-time change. CMS has confirmed it will recalculate the efficiency adjustment every three years, meaning future reductions are already built into the policy.
Change 3: The Site-of-Service Payment Differential
This is the change that has the most immediate revenue impact for facility-based providers.
CMS finalized a significant revision to how indirect practice expense (PE) RVUs are calculated for services performed in a facility setting. Beginning in 2026, the portion of facility PE RVUs allocated based on work RVUs is reduced to half the amount used for non-facility services.
In plain terms: if you perform the same CPT code in a hospital or outpatient facility versus your own office, you are now paid materially less for the facility version.
As Holland and Knight’s analysis of the final rule explains, this change redistributes payments by increasing compensation for office-based specialties while reducing payments for hospital-based specialties. The impact varies widely by specialty and by the mix of facility versus non-facility services in a practice’s billing volume.
For context, using data from the American College of Cardiology: cardiovascular facility-based services are projected to decline 7%, while non-facility cardiovascular services are projected to increase 5%. Two cardiologists performing identical procedures may now see significantly different reimbursements purely based on setting.
Why Underpayments Are the Silent Revenue Problem You Are Not Watching
Most billing teams track denials. They watch the denial rate, work the appeal queue, and measure how quickly denied claims get resolved. That is good practice.
But underpayments are different. They arrive as accepted claims with payments posted to the account. The system marks them paid. Nobody flags them. And the revenue quietly walks out the door.
With the 2026 Medicare fee schedule introducing new conversion factors, RVU adjustments, and site-of-service differentials, the opportunity for systematic underpayment has increased significantly. Payers do not always update their 2026 reimbursement rates promptly. Fee schedules loaded into billing systems at the start of the year may not reflect all finalized changes. And without a structured comparison process, these gaps go undetected.
This is exactly why a Medicare reimbursement audit is not optional in 2026. It is a financial control measure.
Step-by-Step: How to Audit Your 2026 Medicare Reimbursements
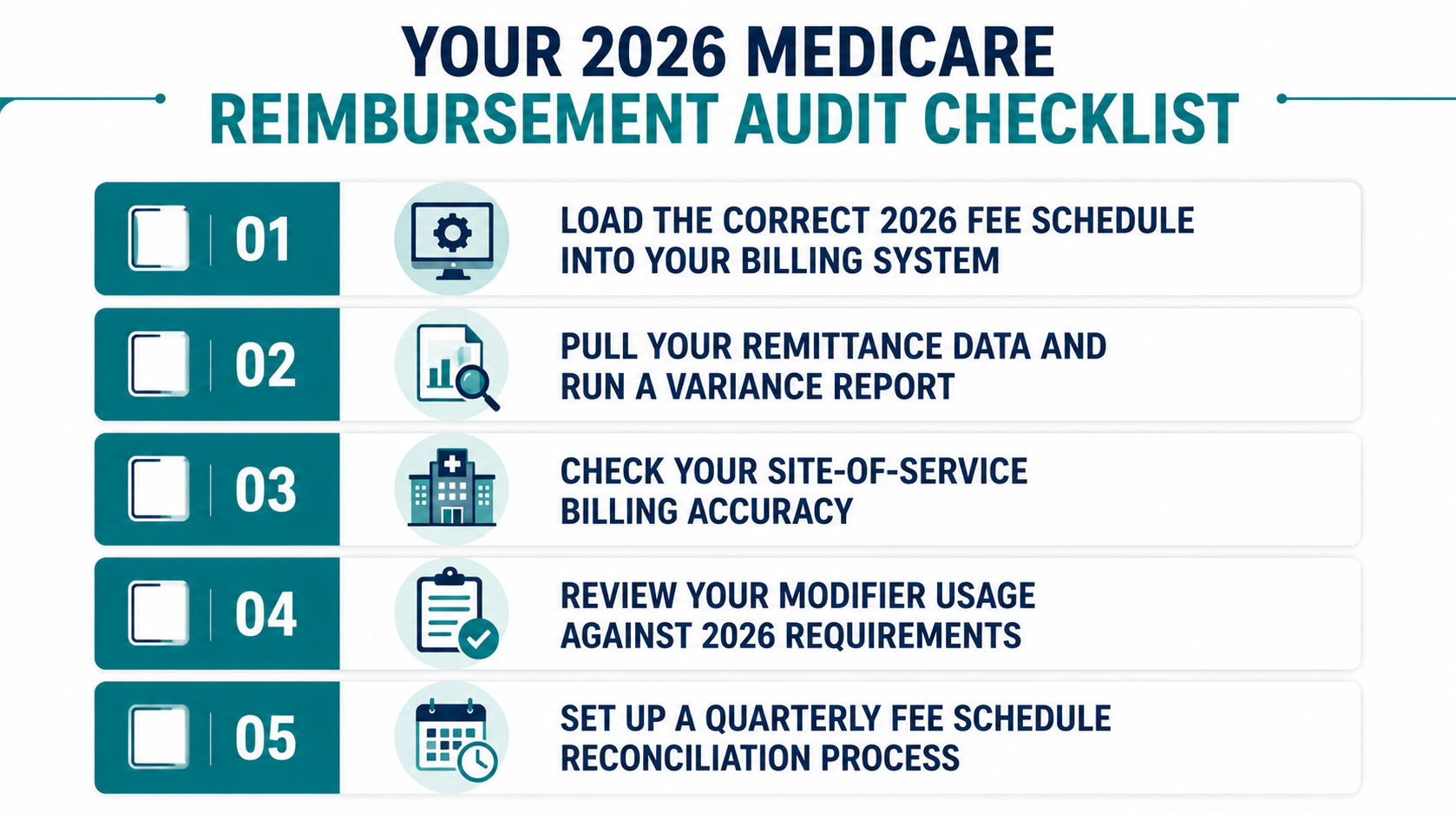
Step 1: Load the Correct 2026 Fee Schedule Into Your Billing System
This sounds obvious. It is not always done.
Your practice management system needs to be updated with the correct 2026 CMS Physician Fee Schedule rates specific to your Medicare Administrative Contractor (MAC) locality. Reimbursement rates vary by geographic location, so national average rates are not sufficient. CMS publishes locality-specific fee schedule amounts in Addendum B of the final rule.
Check that:
- The correct conversion factor is applied based on your APM status ($33.57 for QPs, $33.40 for others)
- Your top 20 to 30 billed CPT codes are updated with the correct 2026 RVU values
- Facility and non-facility rates are loaded separately for CPT codes you bill in both settings
Step 2: Pull Your Remittance Data and Run a Variance Report
For a meaningful audit, pull at least 90 days of Medicare remittances and compare actual payment amounts against your loaded fee schedule rates by CPT code.
You are looking for the gap between what you were paid and what you should have been paid. Even small variances at high claim volume add up fast. Focus on:
- Your highest-volume CPT codes (where small underpayments compound across the most claims)
- CPT codes performed primarily in a facility setting (highest exposure under the new site-of-service differential)
- Non-time-based procedural codes subject to the efficiency adjustment
If you find a consistent underpayment pattern on specific CPT codes or from specific payers, that is a billing or system configuration issue that needs to be corrected and appealed.
Step 3: Check Your Site-of-Service Billing Accuracy
The 2026 site-of-service differential means your place-of-service (POS) code on every claim needs to be accurate. Billing a service with POS 11 (office) when it was actually performed at POS 22 (outpatient hospital) will result in the wrong rate being applied, and potentially a compliance exposure if discovered in an audit.
Review a sample of your facility-based claims and confirm:
- POS codes correctly reflect where each service was rendered
- Facility versus non-facility rates are being applied based on the actual billing setting
- Providers who split time between office and hospital have claims categorized correctly by location
Step 4: Review Your Modifier Usage Against 2026 Requirements
Modifiers continue to be one of the most common sources of underpayment and rejection in Medicare billing. With new 2026 CPT and RVU updates, some modifiers have changed in their application requirements.
Key modifiers to review include global surgery package exceptions, assistant-at-surgery modifiers, and the bilateral procedure modifier. A modifier error does not always produce an outright denial. Sometimes it produces a payment reduction that gets posted and accepted without question.
Have a certified coder review modifier usage on your top 20 billed procedure codes against the 2026 CMS guidelines.
Step 5: Set Up a Quarterly Fee Schedule Reconciliation Process
An audit is not a one-time event. The 2026 CMS fee schedule changes take effect for services rendered on or after January 1, 2026, but payers do not always update their systems immediately. Medicare Administrative Contractors can have a short lag in implementing fee schedule updates.
Run a formal fee schedule reconciliation quarterly. Compare your loaded rates against the current published CMS fee schedule for your locality. Flag any discrepancy of $1 or more per unit for your top-volume codes and initiate a payment inquiry with the MAC if a systemic underpayment is confirmed.
Specialty-Specific Watch Areas for 2026
The impact of the 2026 Medicare fee schedule is not uniform. Depending on your specialty and billing mix, your risk profile is different.
Here is a quick reference by specialty category:
- Procedural specialties (orthopedics, neurosurgery, interventional radiology):
High exposure to both the efficiency adjustment and the facility PE cut. Run your audit with priority on facility-billed procedural codes. - Office-based specialties (primary care, psychiatry, general internal medicine):
Likely to see modest gains from the conversion factor increase and improved non-facility PE rates. Audit should still confirm rates are loaded correctly. - Infectious disease, hematology/oncology:
According to the AMA analysis, 81% of infectious disease physicians face cuts of 5% or more. Audit is critical. Confirm RVU values by code are correct in your system. - Cardiology:
Facility-based cardiology services are projected to decline 7%, while non-facility cardiovascular services are projected to increase 5%. If you practice in both settings, your overall impact depends entirely on your billing mix.
- Sleep medicine:
CMS reduced indirect PE RVUs for facility-based services by 7% while increasing non-facility PE by 4%, according to the AASM 2026 fee schedule analysis. Hospital-based sleep labs face the steepest hit.
What ProMantra Helps You Do With This Information
Understanding the 2026 Medicare fee schedule changes is one thing. Applying that knowledge accurately across thousands of claims per month is another.
At ProMantra, our revenue cycle management team works with healthcare providers to run structured reimbursement audits, load and validate updated fee schedules by locality and payer, and identify underpayment patterns before they compound into significant revenue loss. We track CPT-level reimbursement variances, cross-check against CMS Addendum B rates, and flag any systematic gaps for correction and appeal.
If your practice has not completed a 2026 Medicare fee schedule audit yet, now is the right time. The longer underpayments sit uncorrected, the harder recovery becomes.
Frequently Asked Questions
- What is the 2026 Medicare conversion factor and how does it affect my reimbursements?
The 2026 Medicare Physician Fee Schedule established two conversion factors for the first time: $33.57 for qualifying APM participants and $33.40 for all other clinicians. Every Medicare service payment is calculated by multiplying the service’s RVU value by the applicable conversion factor. If your billing system has not been updated with the correct 2026 rate for your APM status, your reimbursement calculations will be inaccurate, which can lead to missed underpayment appeals.
- What is the 2026 efficiency adjustment and which specialties are most affected?
The efficiency adjustment is a new 2.5% reduction to work RVUs for non-time-based services, finalized by CMS in the 2026 MPFS final rule. It is based on the assumption that certain procedures have become faster and less resource-intensive due to technology. Specialties with high volumes of non-time-based procedural codes, such as orthopedic surgery, interventional radiology, and neurosurgery, face the most significant impact. The adjustment is set to be recalculated every three years.
- How does the 2026 site-of-service differential affect providers who work in both office and hospital settings?
Beginning in 2026, facility-based services have a reduced indirect practice expense allocation, resulting in lower reimbursements for services rendered in a hospital or outpatient facility compared to an office setting. Two providers performing the same CPT code in different settings will be paid materially different amounts. For providers who split time between settings, your overall financial impact depends on how much of your volume is facility-billed versus office-billed.
- How often should a practice run a Medicare reimbursement audit in 2026?
At minimum, you should run a fee schedule validation check when the new year’s rates take effect, and then a formal payment variance audit quarterly. Given the number of changes in the 2026 Medicare fee schedule, the first audit should be a priority if it has not been completed. CMS notes that Medicare Administrative Contractors may not always update reimbursement rates immediately, which means systematic underpayments can accumulate before anyone notices.
Conclusion: The 2026 Fee Schedule Is Already in Effect. Your Audit Should Be Too.
The 2026 Medicare fee schedule is one of the most structurally complex updates in recent years. A headline 2.5% conversion factor increase coexists with an efficiency adjustment that reduces it, a site-of-service cut that changes facility-based reimbursements significantly, and specialty-level impacts that range from meaningful gains to cuts exceeding 5%.
The practices that protect their revenue in this environment are not the ones waiting for underpayments to surface in their AR aging report. They are the ones running structured audits, comparing actual remits against updated fee schedule rates, and fixing discrepancies before they compound.
Your billing team has everything it needs to start this audit today. Pull your top CPT codes, compare your payments against the 2026 CMS fee schedule for your locality, check your site-of-service billing accuracy, and review modifier usage against current requirements.
If you want expert support in running this audit or updating your fee schedule configurations, ProMantra’s RCM team is ready to help you identify exactly where your reimbursements may be falling short.
Do not let the 2026 fee schedule changes quietly reduce what you have already earned.
Contact ProMantra today to schedule a Medicare reimbursement audit and make sure every dollar billed comes back to you.