If you are a healthcare CFO, you already know the revenue cycle is complex. What you may not know is exactly how much money is slipping through the cracks every single month.
According to a 2025 Kodiak Solutions analysis, hospitals and health systems lost more than $48 billion in net revenue in 2025 to final denials and uncollected patient balances. That is a 25% increase from 2024. And most of that loss was not inevitable. It was preventable.
The question is: are you asking your RCM team the right questions?
This blog breaks down what revenue integrity audits actually look like in practice, what CFOs should be demanding from their RCM teams today, and how leading healthcare organizations are using structured audit programs to protect their margins. If you want to stop reacting to financial leakage and start preventing it, you are in the right place.
What Are Revenue Integrity Audits, Really?
Let us get past the jargon.
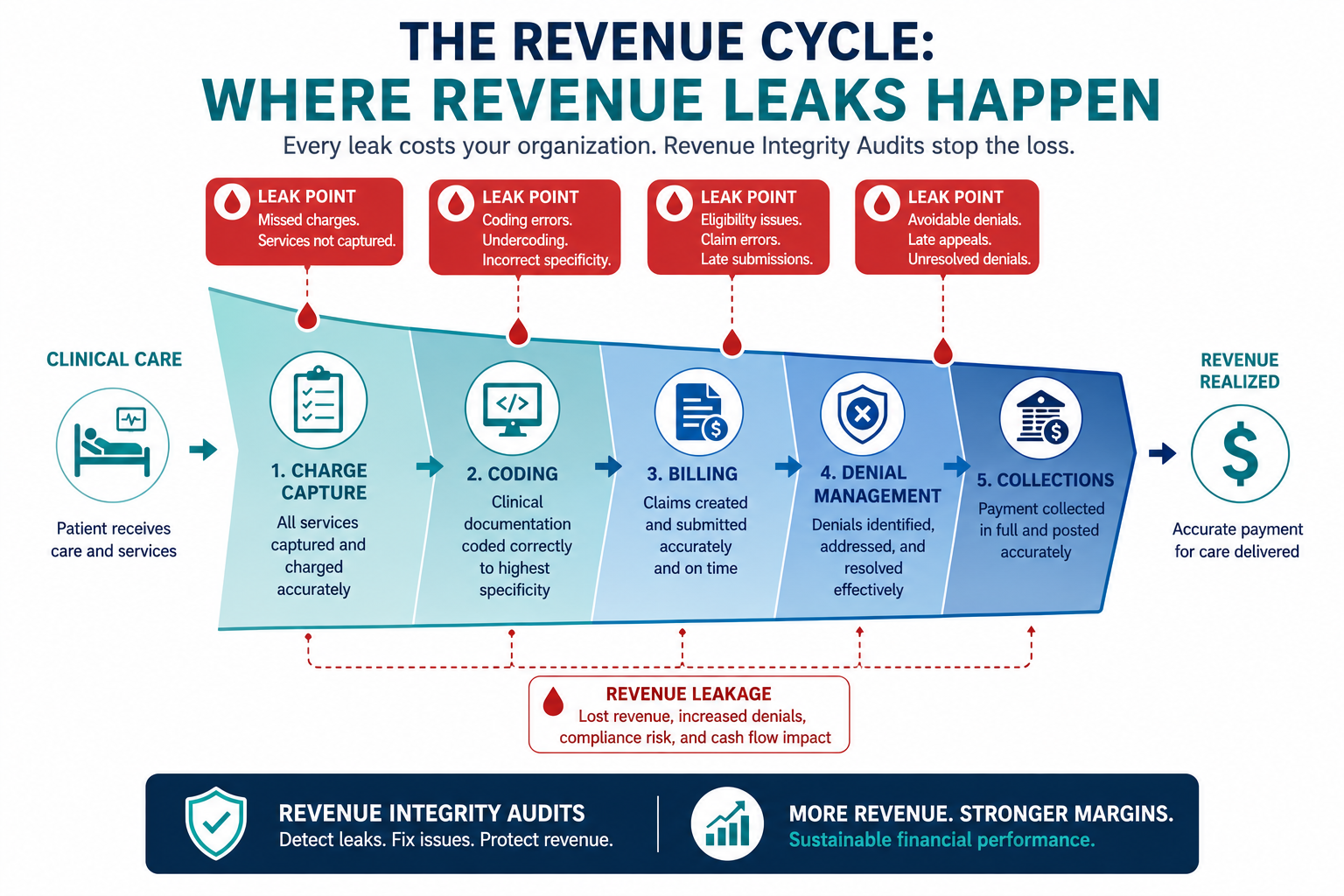
Revenue integrity is the discipline of making sure every clinical service your organization delivers is accurately documented, correctly coded, properly billed, and fully reimbursed. It sits between clinical care and your final payment. When it works, every earned dollar is collected. When it fails, that money disappears into denial queues, underpayments, and missed charges.
Revenue integrity audits are the formal reviews that evaluate whether your revenue cycle is operating the way it should. Think of them as a diagnostic scan of your financial health. They examine:
- Charge capture accuracy (were all services actually billed?)
- Coding correctness (is your clinical documentation supporting the codes submitted?)
- Denial patterns (are the same issues triggering denials repeatedly?)
- Payer contract compliance (are you being paid at the contracted rate?)
- Compliance risk (are there patterns that could trigger OIG or RAC scrutiny?)
NAHRI defines revenue integrity as preventing the recurrence of issues that cause revenue leakage or compliance risk through effective, replicable processes and internal controls that can withstand audits at any point in time.
In plain terms: revenue integrity audits are not just a compliance exercise. They are a financial performance strategy.
The Numbers That Should Have Every CFO Paying Attention
The data from 2024 and 2025 makes one thing very clear: the financial exposure from weak revenue integrity is accelerating.
Here is what the numbers show:
- $48 billion+ in net revenue was lost by over 2,300 hospitals in 2025 to final denials and bad debt
- Initial claim denial rates hit 11.8% in 2024, up from 10.2% in 2020
- Payer audits rose 30% year-over-year in 2025, putting providers under unprecedented scrutiny
- Over 40% of healthcare organizations lose 10% or more of annual revenues to leakage, and 23% do not even know how much they are losing
- Organizations without a formal revenue integrity program typically lose 3 to 8% of net collectible revenue to revenue leakage and most CFOs don’t realize it until it’s too late.
On the flip side, HFMA research found that organizations with dedicated revenue integrity departments reported a 68% improvement in net collection rates.
The difference between those two outcomes? Structured, proactive revenue integrity audits.
5 Things CFOs Should Non-Negotiably Demand from Their RCM Teams
Your RCM team should not be waiting for you to discover problems. They should be finding them first. Here is what you should expect from any high-performing RCM function.
1. A Structured, Recurring Audit Schedule
One-time audits are not enough. If your team only conducts a coding review once a year, you are essentially driving with no dashboard lights.
A mature revenue integrity audit program runs on a defined calendar:
- Monthly: High-risk claim audits, top denial drivers by payer, charge capture reconciliation
- Quarterly: Coding accuracy reviews by service line, provider-level performance reports, payer underpayment analysis
- Annually: Full-scope compliance audit, CDI (Clinical Documentation Improvement) program assessment, benchmark comparison against industry standards
The MGMA recommends designing audits around strategic initiatives including performance measures, validation of coded claims, and adherence to policies and procedures to ensure compliance.
Ask your RCM team: when was the last time a scheduled audit surfaced a billing issue before a payer did?
2. Charge Capture and Coding Accuracy Reporting
This is where most organizations bleed money quietly.
Charge capture failures happen when a service is delivered but the charge never makes it to the claim. Coding errors happen when the clinical complexity of a case is under-documented or miscoded. Both result in the same thing: you delivered care and did not get paid for it.
The American Medical Association estimates that approximately 12% of medical claims contain coding errors that lead to denials or payment delays. Overcoding triggers audits; undercoding leaves legitimate revenue on the table.
What to demand from your RCM team:
- A charge reconciliation report that compares delivered encounters against billed charges
- Coding accuracy rates by provider and department
- A breakdown of undercoded vs. overcoded claims
- A CDI workflow that catches documentation gaps before claims are submitted
At ProMantra, revenue integrity audits always begin with a charge capture and coding accuracy diagnostic. We map leakage at the source before recommending any process change.
3. Denial Root Cause Analysis, Not Just Denial Rates
Most RCM reports tell you your denial rate. That is not enough.
A 12% denial rate is just a number. What matters is why denials are happening and whether the same root causes keep repeating. Treating denials as isolated events instead of systemic signals is one of the most expensive mistakes an RCM team can make.
Your RCM team should deliver:
- Denials segmented by payer, service line, provider, and denial reason code. ProMantra’s denial management workflow includes root cause classification and corrective action plans.
- A root cause classification that distinguishes between front-end failures (eligibility verification, prior authorization), mid-cycle failures (coding, documentation), and back-end failures (billing and follow-up)
- A denial trend report showing whether specific issues are improving or compounding over time
- A re-audit process after corrections are implemented to confirm the fix actually worked
The MDaudit 2025 Benchmark Report makes this point clearly: reactively fixing denials after they occur is costly and unsustainable. The shift is from retrospective denial management to predictive, pre-submission revenue protection.
If your RCM partner only sends you a denial rate without root cause context, you are missing the most valuable part of the data.
4. Real-Time Dashboards, Not Monthly PDF Reports
By the time a monthly PDF arrives on your desk, the problems described in it are already four to six weeks old. In a fast-moving reimbursement environment, that lag is expensive.
The 2024 HFMA/Guidehouse Revenue Cycle Survey identified analytics and reporting as top stressors for revenue cycle departments, largely due to the gap between operational details and executive vision. CFOs need net reimbursement data, denial recovery metrics, and risk-adjusted revenue projections, not raw operational summaries.
What modern revenue integrity audits should produce:
- A live dashboard that surfaces denial trends, payer performance outliers, and coding accuracy metrics proactively. ProMantra delivers real-time performance dashboards designed for CFO-level visibility.
- KPIs tied to your enterprise financial goals (EBITDA, net revenue) not just billing productivity.
- Alerts when a specific metric crosses a performance threshold.
- Benchmarking data that compares your performance against industry top-quartile organizations.
Top-performing health systems consistently outperform peers on denial prevention precisely because they act on real-time data, not lagging reports. The top 25% of organizations maintained a final denial rate of just 1.6% compared to a median of 2.7%.
5. Payer Contract Compliance and Underpayment Tracking
This one often goes undetected for months, sometimes years.
Payer underpayments occur when an insurance company reimburses you at a rate below what your negotiated contract specifies. Without systematic contract reconciliation built into your revenue integrity audit process, these discrepancies pile up silently.
Risk-based pre-bill audits increased 30% in 2025, and payer behavior is increasingly variable by plan type. Medicare Advantage plans had initial and final denial rates more than double the rates for traditional Medicare, making payer-specific tracking a necessity, not an option.
Demand from your RCM team:
- A payer contract matrix that tracks contracted rates against actual payments received
- Monthly underpayment recovery reports
- Payer-specific audit results that flag contract variance before it accumulates
- An escalation process for consistent underpayment patterns
Red Flags Your RCM Team Is Falling Short on Revenue Integrity
Not every RCM team operates with the same level of rigor. Here are warning signs that your current setup may be costing you:
- Your team only conducts coding reviews annually or when a payer audit is triggered
- Denial reports show rates but no root cause breakdowns
- You receive monthly summaries but have no visibility into real-time performance
- Underpayment tracking is not part of your standard reporting
- Your charge reconciliation process is manual or inconsistent
- There is no structured CDI program connecting clinical documentation to billing outcomes
- Audit findings surface the same issues cycle after cycle with no corrective action tracking
How ProMantra Approaches Revenue Integrity for Healthcare CFOs
At ProMantra, we understand that CFOs do not have time for vague reports and reactive fixes. Our revenue cycle management services are built around a structured, audit-first approach that gives healthcare finance leaders the clarity and control they need.
Our revenue integrity audit process covers:
- Charge capture and coding accuracy reviews by provider and department
- Denial trend analysis with root cause classification and corrective action plans
- Payer contract reconciliation to identify and recover underpayments
- CDI integration to close the gap between clinical documentation and billing accuracy
- Real-time performance dashboards designed for CFO-level visibility
- Compliance monitoring aligned with OIG, CMS, and HIPAA requirements
We work with healthcare providers across specialties, bringing the depth of expertise needed to handle both the complexity of payer-specific rules and the operational discipline that revenue integrity demands.
Whether you are looking to plug immediate revenue leakage or build a long-term audit program that protects your financial performance, ProMantra’s RCM team is ready to partner with you.
Frequently Asked Questions
Q1: How often should revenue integrity audits be conducted?
The best practice is to run audits at multiple intervals. High-risk claim audits and charge reconciliation should happen monthly. Coding accuracy reviews and payer performance analysis should happen quarterly. A full compliance and CDI audit should be conducted at least annually. The frequency can increase based on your denial rate, service line complexity, and payer mix.
Q2: What is the difference between a revenue integrity audit and a standard billing audit?
A billing audit typically reviews whether claims were submitted correctly. A revenue integrity audit is broader. It examines the entire pathway from charge capture and clinical documentation through to final reimbursement. It identifies systemic issues upstream of billing, like CDI gaps, charge capture failures, and payer contract variances, not just claim submission errors.
Q3: What are the most common issues uncovered during revenue integrity audits?
The most frequently identified issues include charge capture failures (services billed below what was delivered), coding errors from documentation that does not support the assigned codes, denial patterns that repeat without root cause resolution, payer underpayments from contract rate variances, and compliance drift in areas like modifier usage and medical necessity documentation.
Q4: Can revenue integrity audits help protect against OIG or RAC audits?
Yes. Proactive revenue integrity audits create an internal compliance trail that demonstrates good-faith oversight. The updated CMS 60-Day Overpayment Rule (effective January 1, 2025) requires providers to report and return identified overpayments within 60 days. Organizations with continuous internal audit workflows are far better positioned to respond to external scrutiny and avoid False Claims Act exposure than those that audit reactively.
Take Control of Your Revenue Integrity Today
Your revenue cycle is either working for you or against you. And the only way to know for certain is through structured, consistent revenue integrity audits that surface the truth before payers or regulators do it for you.
ProMantra helps healthcare CFOs build RCM programs that go beyond billing. We deliver audit-driven insights, real-time performance visibility, and corrective action plans that protect your margins and strengthen your compliance posture.
Ready to stop leaving revenue on the table?
Schedule a free Revenue Integrity Assessment with ProMantra today and find out exactly where your RCM team is falling short and what it will take to fix it.