If your practice has invested in RCM automation and still finds your billing team buried in rework, your denial rate has not moved, and your cost to collect keeps climbing, you are not alone.
Across the country, healthcare providers have spent real money on automation tools, workflow software, and AI-powered billing platforms. Many of them are getting modest improvement at best, and some are seeing no measurable change at all.
According to a 2026 Healthcare AI Trends survey, 60% of healthcare executives say they have not yet implemented AI or automation meaningfully in their revenue cycle operations. Of those who have, just 2% say they have fully or mostly integrated these technologies across their RCM operations.
The problem is not that automation does not work. The problem is that most practices are using the wrong kind of automation for the complexity of the problems they are trying to solve.
In this blog, you will learn exactly why traditional RCM automation keeps hitting a ceiling, what the six most common failure modes look like in practice, and how agentic AI in healthcare is fundamentally different in the way it handles the same challenges.
The Automation Investment That Did Not Pay Off
When most practices talk about RCM automation, they mean one of a few things: eligibility verification bots, claims scrubbing tools, automated denial routing, or rule-based prior authorization workflows. Explore our healthcare automation solutions to see how a workflow-first approach changes that.
These tools work. But only within a narrow set of conditions.
RCM AI tools typically fail at scale because they are built as standalone products rather than embedded, workflow-aware solutions. Poor data quality, fragmented EHR integration, and a product-first rather than workflow-first approach are the main culprits for failure.
In other words, the tool does its job. But the system around it was never built to support it.
When payer rules change, when a patient has a non-standard insurance situation, when a denial comes back with an unusual remark code, the automation hits a wall. A human steps in. And that human is your billing team, doing the same rework your automation was supposed to eliminate.
This is the failure pattern most providers recognize but rarely diagnose clearly. Let us break it down.
6 Reasons Your RCM Automation Keeps Hitting a Ceiling
1. It Follows Rules. Payers Do Not.
Traditional RCM automation is rule-based. It does exactly what you tell it to do, nothing more. If the eligibility check returns a flag, it routes to a worklist. If a claim is denied with code CO-4, it queues for appeal.
The problem is that payer behavior does not follow consistent rules. Payers change their coverage criteria, update their authorization requirements, and alter their claims adjudication logic without warning. A rule-based system has no way to adapt.
Unlike traditional automation, which follows fixed rules for repetitive tasks, agentic AI can make complex decisions and orchestrate across AI agents to provide more cohesive, seamless automation.
Every time a payer updates their policy, your rule-based automation becomes slightly less accurate. Over time, those gaps compound into a significant denial problem.
2. It Operates in Silos, Not Across the Full Revenue Cycle
Most automation tools are deployed as point solutions. One tool handles eligibility. Another handles coding. A third routes denials. None of them talk to each other.
While about 46% of hospitals and health systems now use AI in their RCM operations, the number of providers using automation and AI in revenue cycle management has actually declined from 62% in 2022 to 31% in 2024, suggesting implementation challenges around accuracy and reliability.
When tools do not share data, they cannot connect the dots. A coding error that originated in documentation is invisible to the denial management tool. The front-end eligibility gap that caused a back-end authorization failure is never traced back to its source. Each tool solves its piece of the puzzle, but the bigger revenue leak goes undetected.
3. It Cannot Handle Exceptions, and Healthcare Is Full of Them
A large portion of revenue cycle work involves situations that fall outside normal parameters. A patient with Medicare Advantage through a plan your system does not recognize. A prior authorization for a service that requires clinical documentation in a non-standard format. A denial that uses a payer-specific reason code your routing logic does not account for.
By directing human expertise toward the cases that truly require it, organizations reduce wasted effort and improve yield without increasing headcount. AI does not need to replace decision-making to be valuable; it just needs to sharpen it.
Traditional automation either forces exceptions to a human queue, which recreates the workload problem, or it mishandles them entirely, which creates a denial or underpayment problem. There is no middle ground. Eliminating revenue leakage with RPA requires a layer of intelligence that sits above static rule sets and acts on the exceptions that matter most.
4. It Gives You Alerts, Not Actions
Many automation platforms are built around dashboards. They surface the problem. They tell you the denial rate is up 3%. They flag that authorization turnaround time has slipped. They show you the trend line.
But they do not fix anything.
Your billing team still has to log in, review the alert, investigate the root cause, take the corrective action, document it, and move on to the next one. The automation improved visibility. It did not reduce work.
This is one of the most common sources of frustration for RCM leaders who invested in automation and felt no meaningful relief in their day-to-day operations.
5. It Was Built for Yesterday’s Volume and Complexity
The revenue cycle is getting harder every year. Initial claim denials hit 11.8% in 2024, up from 10.2% just a few years earlier. Meanwhile, 73% of providers say claim denials are increasing, compared to 42% in 2022.
The tools most practices deployed were designed for a simpler billing environment. The payer mix was more predictable. The authorization rules were less intricate. The volume of denials was lower.
As complexity has grown, static automation tools have not kept pace. They were configured for a baseline that no longer exists.
6. It Was Never Integrated With Clinical Workflows
Billing problems that start in the clinical record cannot be fixed by a billing tool.
When a provider’s documentation does not support medical necessity, when a diagnosis code does not map to the service billed, or when a clinical note is missing information required for a specific payer, the problem was created before the claim was ever generated.
Automation tools that sit only in the billing department have no way to address these upstream issues. They can catch some mismatches at claims scrubbing. But they cannot reach back into the clinical workflow to prevent them at the source.
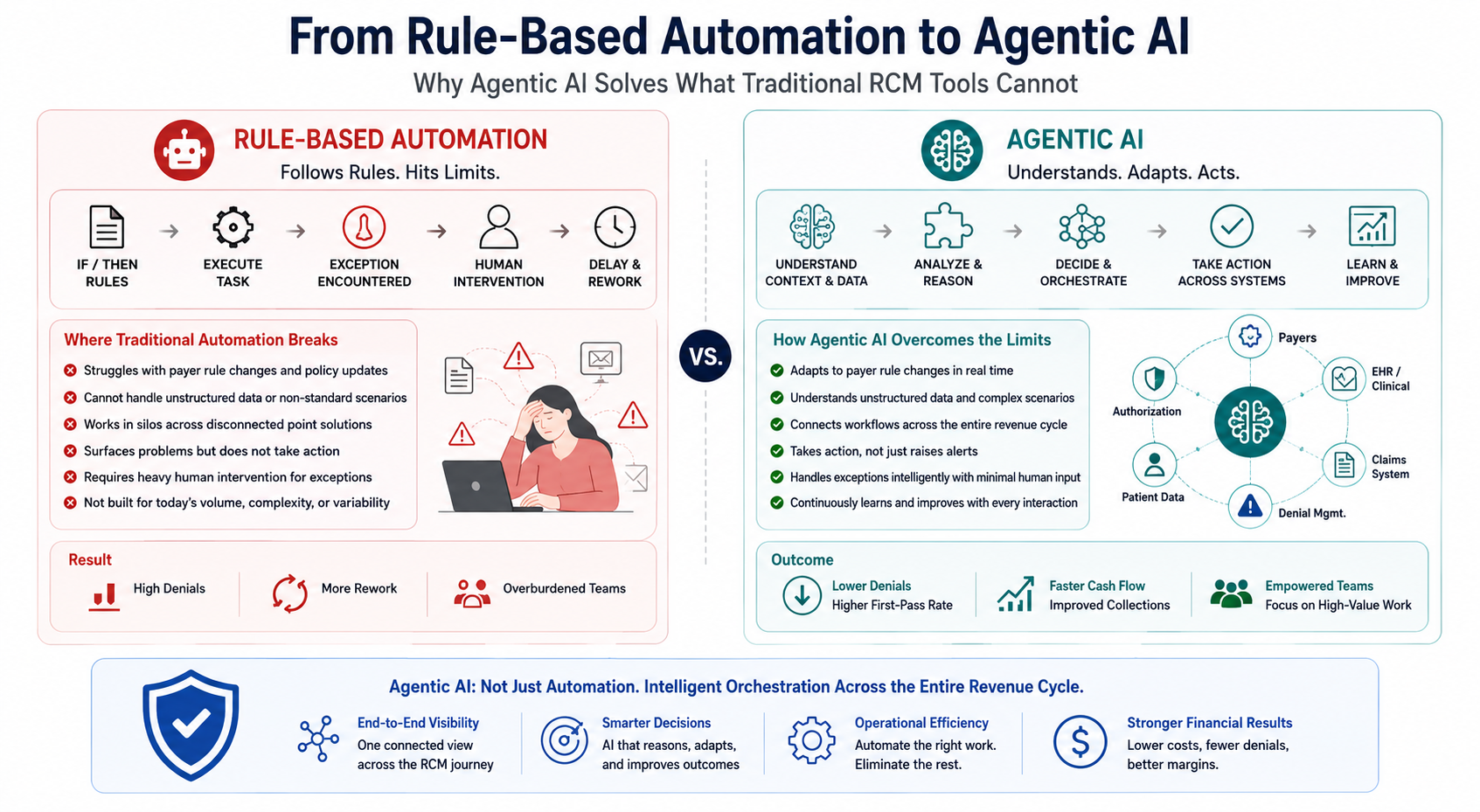
What Agentic AI Does Fundamentally Differently
Agentic AI is not a better version of the same tool. It represents a different architecture entirely.
Agentic AI systems do not merely assist human staff. They autonomously execute multi-step RCM tasks, reasoning across clinical records, payer rules, and outcomes data, with human oversight reserved for flagged exceptions.
Here is how that plays out across the six failure modes described above.
It Adapts to Payer Behavior, Not Just Payer Rules
Where rule-based automation applies static logic, agentic AI learns from claims outcomes over time. It builds a model of how each payer behaves based on your actual submission and payment history. When a payer starts denying a previously accepted code combination, the system detects the pattern before it becomes a systemic problem and adjusts its approach.
McKinsey’s January 2026 report “Agentic AI and the Race to a Touchless Revenue Cycle” highlights that denials and appeals have surged to 61% prioritization intent in 2025, signaling that the market has recognized revenue leakage at the back end as the most urgent problem to address.
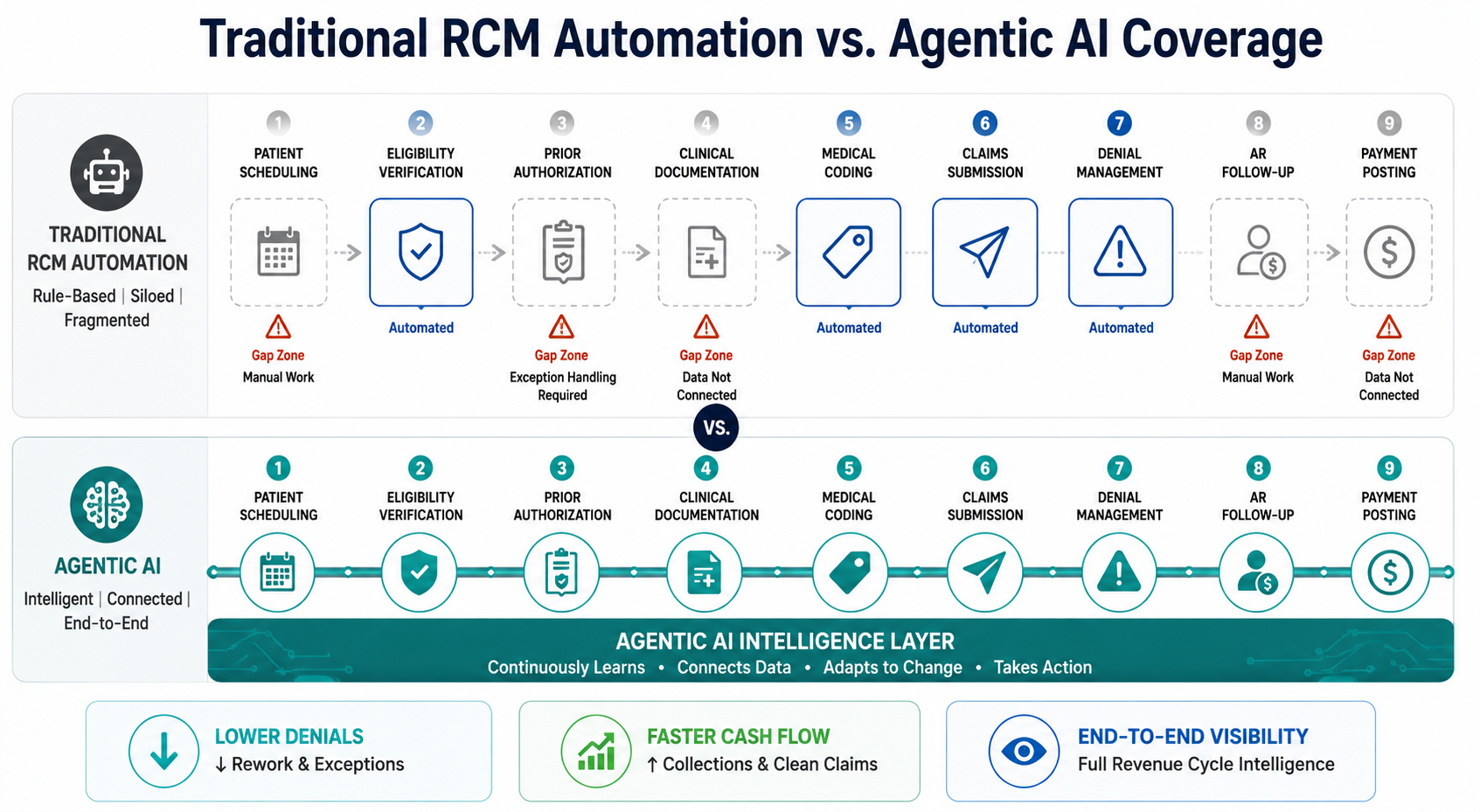
It Works Across the Full Revenue Cycle, Not Just One Stage
Agentic AI is built to operate end to end. It connects front-end eligibility to mid-cycle authorization to back-end denial management in a single intelligence layer. RevvPro is ProMantra’s AI-assisted RCM platform purpose-built for exactly this kind of connected intelligence across the full cycle. When an eligibility issue at scheduling is linked to an authorization failure two weeks later, the system sees the connection and flags both the individual claim and the workflow gap that caused it.
According to McKinsey, using AI to enable the revenue cycle could lead to a 30 to 60 percent reduction in cost to collect, faster cash realization, and a workforce refocused on patient value rather than administrative tasks.
It Takes Action, Not Just Alerts
This is the most operationally significant difference for billing teams.
Agentic AI does not just tell you a denial came in. It reviews the denial, identifies the likely cause, cross-references the payer’s appeal requirements, drafts the appeal with the appropriate documentation, and routes it for human review only when a judgment call is needed. See how this looks in practice in our deep-dive on transforming denial management with AI.The billing team’s involvement shifts from routine execution to exception management.
RCM automation is most valuable when the AI can handle a whole chain of tasks from start to finish without stopping, rather than doing one small copy-paste job at a time.
It Handles Exceptions With Intelligence, Not Just Rules
Because agentic AI reasons across multiple data sources rather than applying static logic, it can handle non-standard situations that traditional automation cannot. It can interpret an unfamiliar denial code by cross-referencing payer policy documentation. It can recognize that a specific claim type for a specific payer historically requires additional documentation and proactively requests it before submission.
Menlo Ventures reported that 22% of healthcare organizations have deployed commercial domain-specific AI applications in 2026, a 7x increase over 2024, with the shift moving from experimentation to embedded strategy.
It Learns Over Time and Gets More Accurate
Traditional automation is as accurate as the rules you give it on day one. Agentic AI improves continuously.
Every denied claim, every successful appeal, every authorization outcome feeds back into its model. It is moving the revenue cycle progressively toward zero-touch claims processing as accuracy compounds over time.
The Real Cost of Staying With Automation That Is Not Working
This is not just a technology discussion. It is a financial one.
Health systems collectively spend more than $140 billion annually on revenue cycle operations, with manual processes, fragmented vendor landscapes, and outdated technologies contributing to high costs, delays, and errors. Nearly 20% of claims on average are denied, and as many as 60% are never appealed, resulting in millions of dollars in lost revenue for the average health system.
For a mid-size practice or health system, the math is uncomfortable. A 10% to 15% denial rate multiplied by average claim values, with 60% of those denials going unappealed, represents a substantial and largely avoidable revenue loss. Automation that merely flags denials without resolving them is not solving this problem. The shift toward real-time claims processing is what closes the gap between visibility and revenue recovery. It is just making it more visible.
HFMA’s Revenue Cycle of the Future survey found that 27% of healthcare organizations are now actively deploying AI at scale across multiple revenue cycle functions, while 53% are conducting pilots. The US RCM market, currently valued at around $90.6 billion, is projected to reach nearly $308 billion by 2030.
The window to act is now. Organizations that move from rule-based automation to agentic AI-driven workflows in the next 12 to 24 months will hold a compounding advantage in cost efficiency, denial rates, and cash velocity over those that wait.
How ProMantra Bridges This Gap for Healthcare Providers
At ProMantra, we understand that most healthcare providers are not starting from zero. You already have billing systems, existing automation tools, and a team that has built workflows around them. A complete overhaul is not realistic for most practices.
Our approach is to build on what you have while introducing the intelligent, adaptive layer that makes your existing investment more effective. We combine experienced RCM professionals with AI-assisted workflows that improve over time. We handle the exceptions your current automation cannot, trace denial patterns back to their upstream source, and create a feedback loop between billing outcomes and front-end workflows.
For practices that have been frustrated by automation that promised more than it delivered, our model works differently. The intelligence is built around your specific payer mix, your patient population, and your service lines, not a generic template applied to every client the same way.
Frequently Asked Questions
- What is the main difference between traditional RCM automation and agentic AI?
Traditional RCM automation applies fixed, rule-based logic to repetitive tasks. It follows pre-set instructions and requires human intervention whenever a situation falls outside those rules. Agentic AI in healthcare operates differently. It reasons across multiple data sources, makes contextual decisions, executes multi-step tasks autonomously, and learns from outcomes over time. The practical difference is that agentic AI can handle exceptions, adapt to payer behavior changes, and take action rather than just surface alerts.
- Why does RCM automation fail even after significant investment?
The most common failure modes are fragmented point solutions that do not share data across the revenue cycle, rule-based logic that cannot keep pace with changing payer policies, and tools that generate insights without taking action. Many automation deployments also sit only in the billing department and cannot address clinical documentation gaps that originate upstream. Without a connected, adaptive system, the fundamental problems persist even with significant automation in place.
- Is agentic AI in healthcare RCM ready for production use right now?
For specific, well-defined RCM functions, yes. Back-end revenue cycle tasks including denials management, AR follow-up, underpayment identification, and authorization tracking are areas where agentic AI is already delivering measurable results in production deployments. Full end-to-end autonomous revenue cycles without any human involvement are further out, but targeted deployment in high-impact areas is viable and valuable today.
- How should a practice evaluate whether their RCM automation is actually working?
Look at three numbers: your first-pass acceptance rate, your denial rate trend over the past 12 months, and the percentage of denied claims that are successfully appealed. If your first-pass rate is below 95%, your denial rate has not meaningfully declined despite automation, or a large share of your denials are going unappealed due to staff capacity, your automation is not solving the core problem. These are the signal metrics that tell you whether your current tools are working or whether you need a different approach.
Conclusion: The Problem Is Not That You Automated. It Is What You Automated.
Most practices that are frustrated with their RCM automation did not make bad technology decisions. They made the right decisions for the automation landscape that existed three to five years ago.
But that landscape has changed. Payers are more complex. Denial rates are climbing. The manual rework that automation was supposed to eliminate has shifted from one part of the cycle to another.
Agentic AI in healthcare is not a replacement for your billing team. It is the upgrade to your automation layer that your billing team has been waiting for. It adapts to what rule-based systems cannot, connects what point solutions keep separate, and acts on what dashboards only display.
The organizations building this capability now will have a structural cost and performance advantage that compounds every year. Those that wait will keep investing in automation that hits the same ceiling.
Is your RCM automation delivering the results you were promised?
Talk to ProMantra’s team about a no-obligation review of your current denial patterns and automation gaps. We will show you exactly where the ceiling is and what it would take to break through it.