If your RCM team spends more time chasing authorizations than it does on care coordination, you are not alone.
Providers and administrative staff spend an average of 13 hours per week on prior authorization tasks, time that could otherwise go toward patients. According to CMS data, prior authorization costs the healthcare industry an estimated $35 billion annually and causes 92% of care delays.
That is the baseline. What makes 2026 a turning point is this: payers are now deploying AI to review and deny claims faster than most providers can respond manually. The old fax-and-phone workflow is not just slow. It is now actively costing you revenue and patients.
AI-driven prior authorization is no longer a pilot program. It is the new operational standard, and providers who do not adapt will feel it directly in their denial rates and AR aging.
This guide is built for healthcare CFOs and RCM leaders who need to understand what is changing, why it matters financially, and precisely what to do next.
What the CMS-0057-F Rule Means for Providers Right Now
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) is the single most significant regulatory shift in PA workflow management in over a decade.
The new CMS rule, effective January 2026, requires payers to respond to urgent PA requests within 72 hours and standard requests within seven calendar days. That mandate is already in effect. Payers that do not meet it are already non-compliant.
For providers, the immediate practical reality is that payers must now:
- Provide specific written reasons for every PA denial
- Publicly report their PA approval and denial metrics
- Move toward electronic prior authorization APIs by January 1, 2027
For providers, the Prior Authorization API replaces weeks of faxes and phone calls with an electronic workflow, helping them check requirements and submit requests in minutes.
This is a real shift in leverage, but only if your practice or health system is set up to take advantage of it.
Key Compliance Dates You Cannot Afford to Miss
| Milestone | Deadline |
| Payers must provide specific PA denial reasons | January 1, 2026 (in effect) |
| Payers must publicly report annual PA metrics | March 31, 2026 (in effect) |
| Urgent PA decision turnaround (72 hours) | January 1, 2026 (in effect) |
| Standard PA decision turnaround (7 days) | January 1, 2026 (in effect) |
| Full FHIR-based Prior Authorization API live | January 1, 2027 |
| Patient Access API with PA decision data | January 1, 2027 |
CMS strongly encourages providers to take an active role by participating in FHIR API testing with their EHR vendor and payer partners, with early testing and collaboration essential to ensure seamless, real-world implementation of electronic prior authorization workflows.
Do not wait for 2027 to start preparing. The providers winning this transition started in early 2026.
How AI-Driven Prior Authorization Actually Works
Understanding AI-driven prior authorization is not about knowing the code behind it. It is about understanding the workflow it replaces and what it enables.
Traditional PA meant your staff member pulled up a payer portal, manually entered patient and clinical data, waited hours or days for a response, and then often picked up the phone to follow up. One request at a time. All day.
AI-driven prior authorization works differently. Here is what it actually does:
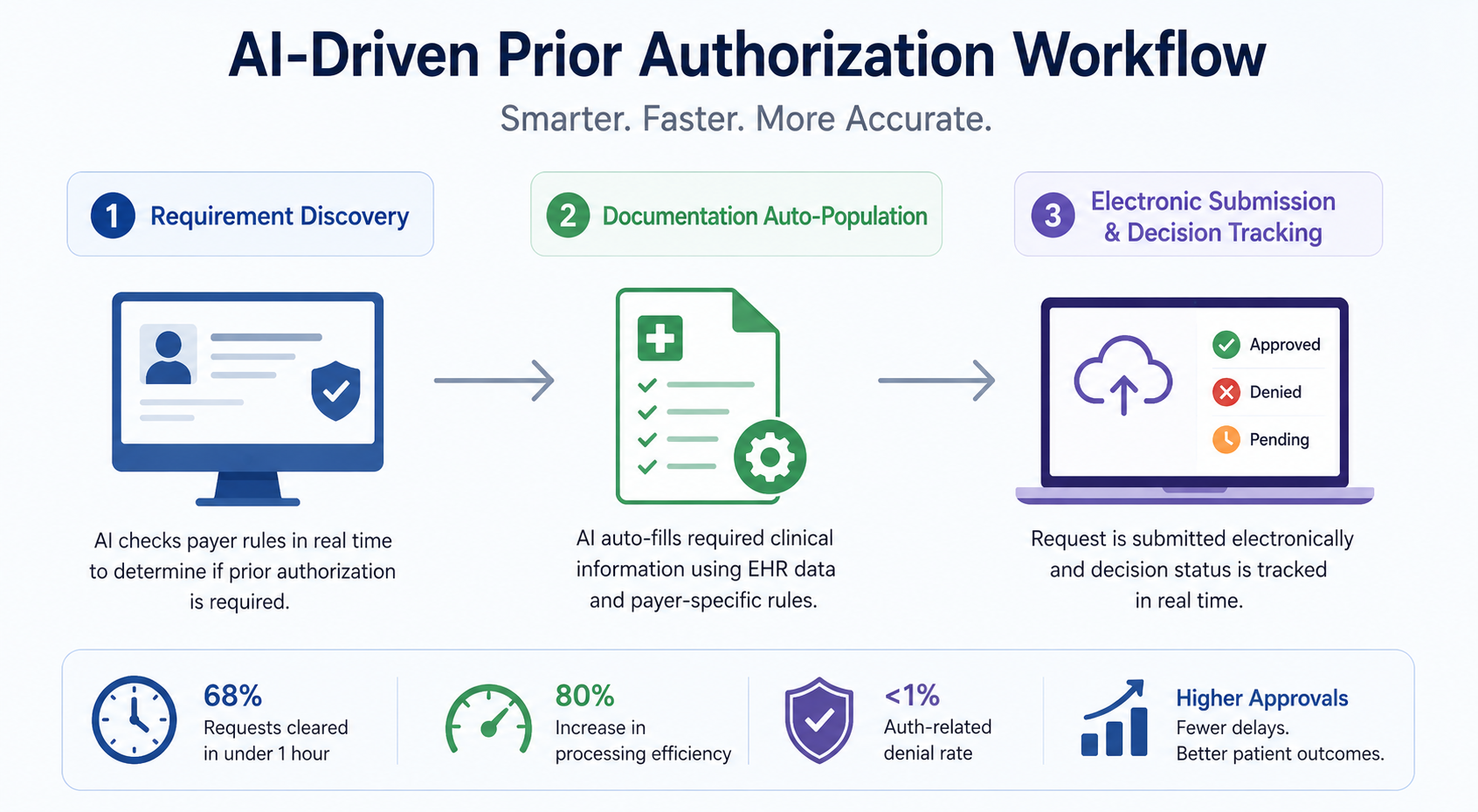
The Three Core Capabilities Powering Automation
- Requirement Discovery (Coverage Requirements Discovery / CRD) When a provider orders a procedure inside the EHR, the system automatically checks whether PA is required for that patient’s specific plan. No manual payer lookup. No missed requirements. The system tells the provider immediately, before the order is placed.
- Documentation Automation (Documentation Templates and Rules / DTR) The AI engine pre-populates the required documentation using structured patient data from the EHR. It knows what each payer’s criteria look like at the procedure level. Leading platforms are pre-trained on over 100,000 payer policies, so they know what each payer requires before submission.
- Electronic Submission and Decision Tracking (Prior Authorization Support / PAS) The system submits the request electronically and tracks the payer’s response in real time. Approvals, denials, and requests for additional information all come back into the EHR automatically.
Smarter workflows eliminate 45% of manual touches and drive an 80% increase in processing efficiency, exactly the kind of performance delivered by end-to-end prior authorization automation platforms built for today’s RCM environment.
The Real Numbers: What Providers Are Losing Without Automation
Let us put revenue impact on the table.
Initial denial rates have climbed to 11.8% industry-wide, and the financial hemorrhage is staggering: $262 billion in medical claims are initially denied every year, with 65% of those denials never resubmitted.
Nearly two-thirds of denied claims are simply abandoned. That is not a billing workflow issue, that is a revenue hole that denial management and AR recovery solutions exist to close.
Prior authorization denials jumped 31% year-over-year in 2026. Industry-wide denial rates now sit at 10 to 15%, and the share of providers reporting denials above 5% has nearly doubled, from 12% to 20%.
The math at the practice level is stark. Individual practices may lose $5 million or more per year without adequate denial prevention, while reworking a denied claim costs $25 or more per claim in staff time.
For a mid-size health system processing thousands of authorizations per month, unchecked PA denials are not an operational inconvenience. They are a material threat to financial performance.
On the flip side, the gains from AI-driven prior authorization are measurable and fast. Care New England, after implementing AI-powered prior authorization automation, recorded an 83% clean submission rate, reduced authorization turnaround times by 80%, decreased time spent on prior authorizations by 2,841 hours, and saved $644,000 in avoided write-offs within one year.
Those are real numbers from a real health system.
Payers Are Already Using AI Against You
This is the part that does not make the vendor brochures.
A nationwide survey of health insurers found that most are already using automated AI systems for prior authorization requests. Roughly 3 out of every 4 plans report they use AI for PA approvals, and a smaller but notable share of 8 to 12% use AI to support PA denials.
When a payer’s AI flags your submission as incomplete, the denial can happen in seconds. Meanwhile, if your team is still manually pulling records and filling out portal forms, your response takes days.
According to the 2026 Revenue Cycle Management Trends survey, 74% of providers reported an increase in prior authorization delays, and 88% said disagreements over claims are preventing their organizations from getting paid.
The imbalance is real. Payers have optimized for speed with AI. Providers who are still running manual PA workflows are competing with a structural disadvantage baked into the process.
MGMA reports 92% of practices have hired or reassigned staff solely for prior authorization. That staff cost compounds as denial volume rises. The irony is that the more denials you receive, the more labor you need to appeal them, unless automation handles both ends.
Healthcare teams using voice AI to handle payer calls have reported cutting their administrative phone work by up to 60%, with one top U.S. insurer noting that AI agent calls shave over one-third off the usual call length.
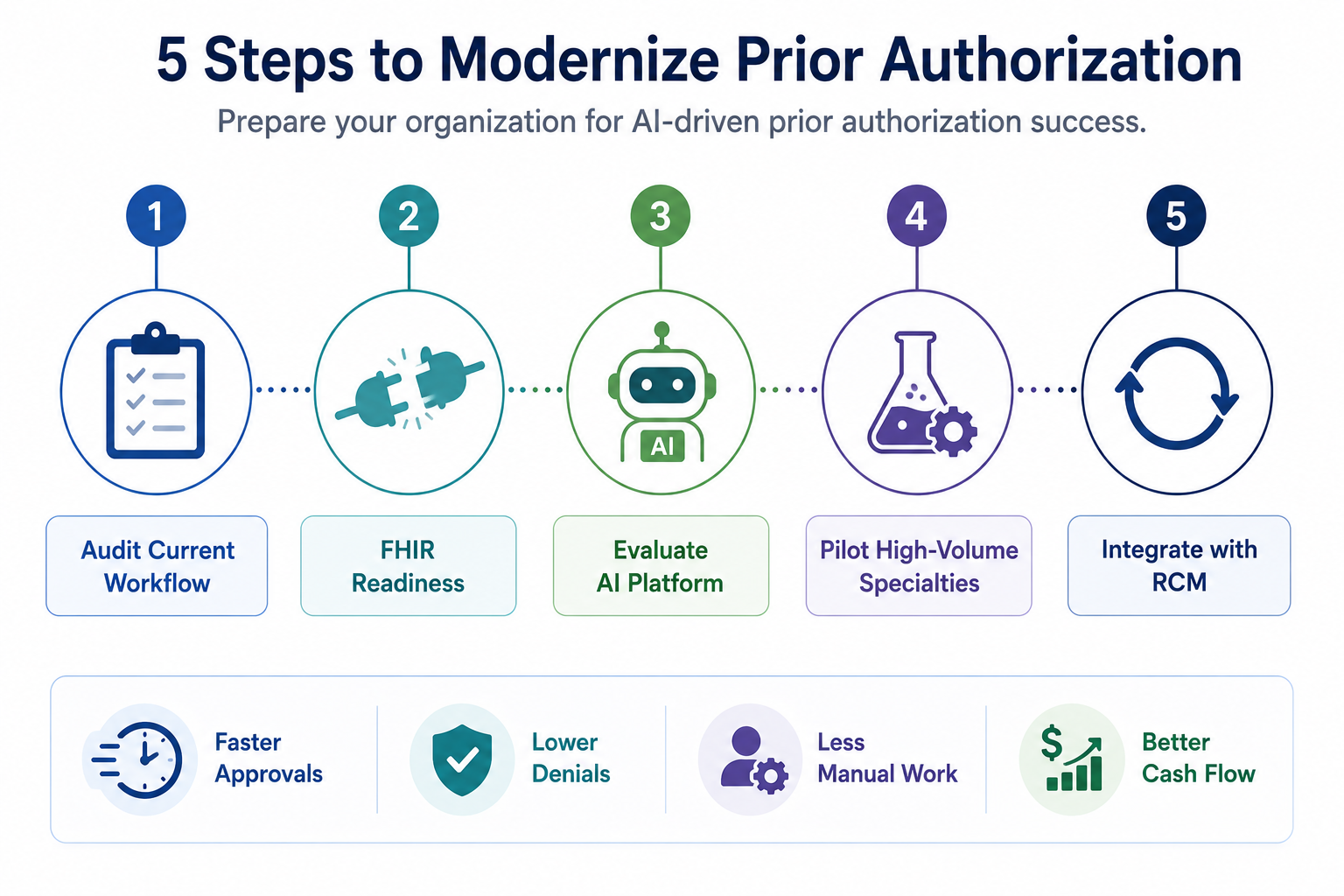
Your 5-Step Action Plan to Modernize Prior Authorization
The shift to AI-driven prior authorization does not have to happen overnight. Here is a practical, phased approach that healthcare operations leaders can execute without disrupting existing workflows.
Step 1: Audit Your Current PA Workflow Before buying technology, map the problem. Identify your top five procedures by PA request volume, your denial rate by payer, and average turnaround time. Baseline data is the foundation for measuring ROI. If your current process already has identifiable bottlenecks, this guide on how to fix prior authorization delays in your practice provides a practical starting framework.
Step 2: Confirm EHR Readiness for FHIR-Based APIs Providers should contact their EHR vendor to learn how and when testing for FHIR-based electronic prior authorization workflows can begin. This collaboration is essential before the 2027 API deadline. Do not wait for your EHR vendor to reach out first.
Step 3: Evaluate AI-Driven Prior Authorization Platforms Look for platforms that offer full coverage of your payer mix, not just the top three. Key capabilities to prioritize:
- Pre-loaded payer policy libraries covering 600 or more payers
- EHR integration with real-time data pull
- CRD, DTR, and PAS capability aligned with CMS-0057-F
- Denial defense and appeal automation
- Analytics dashboard for denial pattern tracking
Providers evaluating purpose-built platforms should explore the RevvPro RCM automation platform, designed to deliver these capabilities within a fully integrated revenue cycle workflow.
Step 4: Pilot with High-Volume, High-Denial Specialties Start where the pain is greatest. Orthopedics, oncology, neurosurgery, and advanced imaging typically carry the highest PA burden. Run a 60-day pilot, track first-pass approval rates, turnaround times, and staff hours saved. The results will make the ROI case for broader deployment.
Step 5: Integrate PA Automation into the Broader RCM Stack AI-driven prior authorization works best when connected to eligibility verification, coding review, and denial management. Siloed tools create gaps. A fully integrated RCM approach, from pre-authorization to claim submission to AR recovery, closes the revenue leak at every stage. For providers ready to take that a step further, learn more about building a denial prevention system that stops revenue leaks before they start.
What to Look for in an RCM Partner for AI-Driven Prior Auth
Not all RCM vendors have built their workflows around the new PA landscape. Here is what separates a capable partner from one who is still catching up.
Regulatory Alignment: Your partner should have active knowledge of CMS-0057-F compliance timelines, FHIR API readiness, and payer-specific documentation requirements that change frequently.
Technology Integration: Look for partners who can connect PA workflows with your EHR and billing systems rather than running a parallel process that creates manual reconciliation work.
Security Credentials: With protected health information (PHI) flowing through PA automation systems, data security is non-negotiable. Verify that any RCM partner holds ISO 27001 and HIPAA compliance certifications as a baseline standard for information security governance.
Denial Analytics: A strong PA partner does not just submit requests. They track patterns, identify payer-specific denial triggers, and feed that intelligence back into pre-submission processes.
Transparent Reporting: You should have real-time visibility into authorization status, denial reasons, and appeal outcomes. Avoid partners who cannot give you this without a custom report request.
How ProMantra Supports Providers Through This Transition
ProMantra is a U.S.-focused revenue cycle management services company that works with healthcare providers navigating exactly this kind of transition.
Our RCM teams are built around the operational realities of AI-driven prior authorization. We support providers with end-to-end prior authorization management, from requirement identification and documentation preparation to electronic submission tracking and denial appeal workflows.
We operate under ISO 27001 and HIPAA compliance standards, so the PHI flowing through your prior authorization processes is handled with the security governance your organization requires.
As the CMS-0057-F mandates continue to take effect and FHIR API requirements approach their 2027 deadline, ProMantra helps providers close the gap between where their workflows are today and where regulatory and payer expectations require them to be.
If prior authorization denials are quietly eroding your revenue, the right time to address it is now, before a backlog becomes a crisis.
Frequently Asked Questions (FAQs)
Q1. What is AI-driven prior authorization, and how is it different from traditional PA? AI-driven prior authorization uses machine learning and real-time EHR integration to automatically identify PA requirements, pre-populate documentation, and submit requests electronically. Traditional PA relies on manual portal entry, phone calls, and faxes. AI-driven systems cut turnaround times from days to hours, reduce first-pass denials, and free clinical staff from administrative bottlenecks.
Q2. Does the CMS-0057-F rule require providers to switch to electronic PA systems? The CMS-0057-F rule primarily places requirements on payers, specifically Medicare Advantage, Medicaid, and CHIP plans, to implement FHIR-based Prior Authorization APIs by January 1, 2027. While providers are not directly mandated, those who do not align their submission workflows with electronic PA systems risk continued delays and denials when payers have fully migrated. CMS strongly encourages providers to begin FHIR API testing with EHR vendors now.
Q3. What kind of ROI can providers expect from automating prior authorization? Real-world results vary, but documented outcomes include first-pass approval rates above 96%, denial rate reductions of 30 to 50% within six months, and significant staff hour savings. Care New England reported over $644,000 in avoided write-offs within one year of implementation. The ROI case is strong, especially for high-volume specialties like orthopedics, oncology, and advanced imaging.
Q4. How does AI-driven prior authorization handle payer policy changes? Leading platforms maintain continuously updated payer policy libraries covering hundreds of payers. Self-learning rules engines adapt to policy changes automatically, reducing the manual updates required when payers revise their clinical criteria. This is a key reason purpose-built PA automation platforms outperform EHR-native workarounds for complex payer mixes.
Q5. Is AI-driven prior authorization secure for handling PHI? Yes, when implemented with the right vendor governance. Look for RCM partners and PA automation vendors who operate under ISO 27001 and HIPAA compliance certifications. These standards ensure that PHI transmitted through PA workflows is governed, encrypted, and audited according to federal and international information security requirements.
Ready to Stop Losing Revenue to Prior Authorization Denials?
AI-driven prior authorization is not a technology upgrade you can schedule for next year. The regulatory shift is already in motion, payers are already operating at AI speed, and denial rates continue to rise for providers who are not keeping pace.
The providers building competitive advantage right now are the ones who have aligned their PA workflows with the new reality: faster decisions, electronic submissions, and data-driven denial prevention built into the front end of the revenue cycle.
ProMantra partners with healthcare providers to implement and manage RCM workflows that are built for today’s prior authorization environment. If you want to see where your current PA process is leaking revenue and how AI-driven solutions can close that gap, let’s talk.
Contact ProMantra today to schedule a prior authorization workflow assessment.