

Most billing teams spend their days reacting. A denial comes in, someone investigates it, they figure out what went wrong, they fix it, they resubmit it, and then the same type of denial shows up again next week.
This cycle is costing you more than you realize.
According to the Healthcare Financial Management Association (HFMA), initial claim denial rates have climbed to nearly 12% in recent years, and a significant portion of those denied claims are never reworked at all, meaning the revenue is simply written off. The American Hospital Association estimates that providers spent around $19.7 billion in a single year fighting back denied claims through appeals.
That’s not a billing problem. That’s a strategy problem.
In this blog, you’ll learn why denial prevention in medical billing outperforms denial management, what the four front-end stages of a prevention-first approach look like, and how to build a practical roadmap your team can actually follow.
Why Denials Feel Inevitable (and Why They’re Not)
There’s a deeply rooted assumption in many provider organizations: denials are just part of the business. Payers are going to push back, so you staff up your AR team and brace for it.
But that assumption is expensive.
The reality is that most denials are preventable. Industry research consistently shows that anywhere from 60% to 90% of claim denials are avoidable with the right front-end processes in place. The problem is that most practices are structured to fix denials after they happen, not to stop them before they start.
This is the difference between denial management and denial prevention in medical billing.
Denial management is reactive. It involves identifying denial codes, drafting appeals, tracking resubmission windows, and recovering what you can. It’s necessary, but it’s expensive and slow.
Denial prevention is proactive. It involves fixing the upstream conditions that cause denials in the first place, before the claim ever leaves your practice. It is faster, cheaper, and far more effective at protecting your bottom line.
The shift doesn’t require you to scrap everything. It requires you to look earlier in the process.
The Four Stages Where Denials Are Actually Born
Most providers think of denial prevention as a billing department task. But by the time a claim reaches billing, the damage is often already done. The root causes live upstream, in four specific stages.
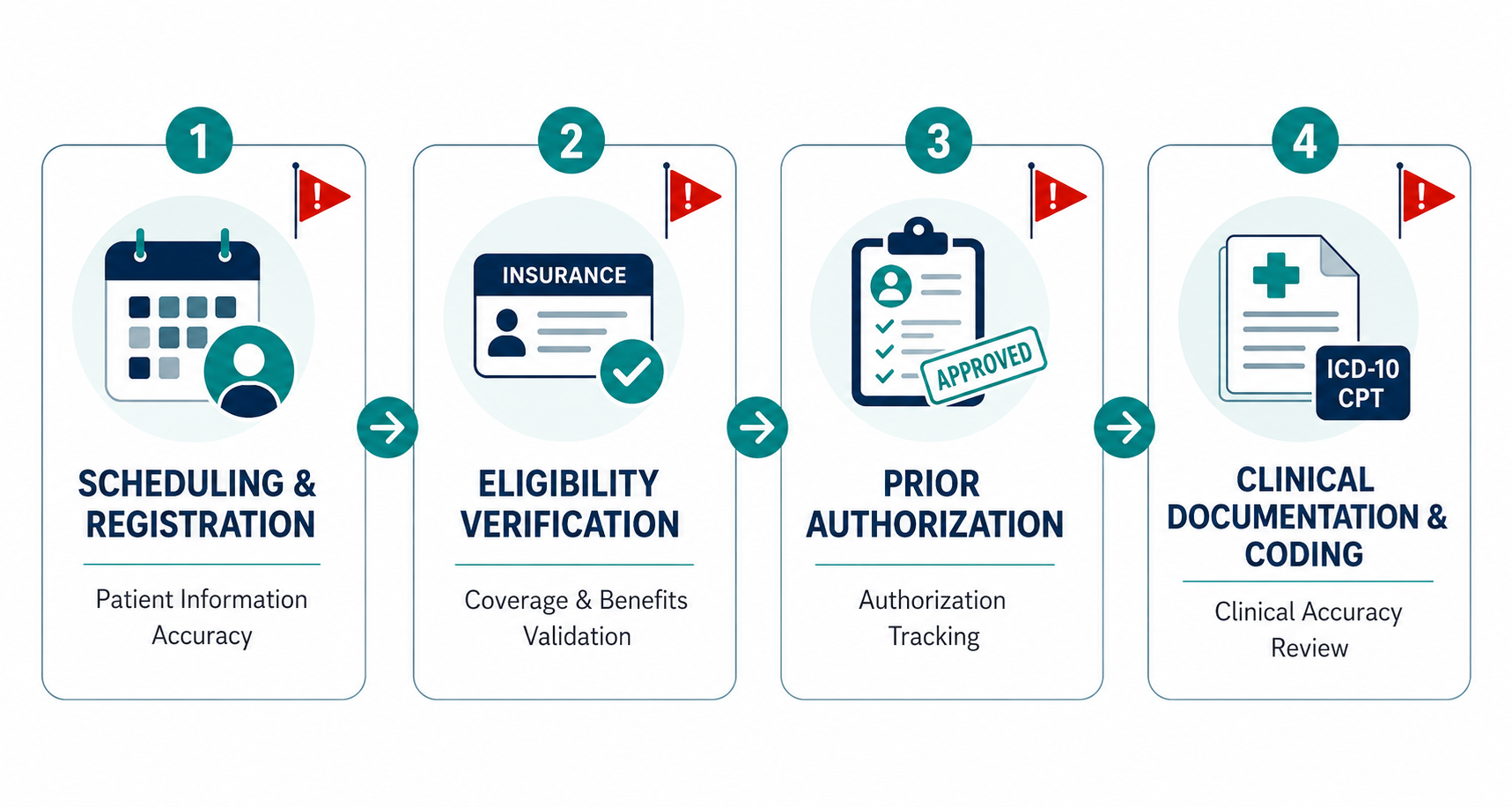
Stage 1: Scheduling and Patient Registration
This is where the denial cycle most often begins, and it’s also the least scrutinized stage.
When front-desk staff collect patient information, small errors have a long tail. A transposed date of birth, a misspelled name, an outdated insurance ID, any of these can trigger a claim rejection that no amount of billing skill will fix quickly.
Common registration errors that drive denials include:
- Incorrect insurance member ID or group number
- Wrong date of birth or subscriber information
- Inactive or outdated policy captured without real-time verification
- Missing secondary insurance when coordination of benefits applies
The fix at this stage is standardizing your intake process. Every patient registration form should be validated against a structured checklist before the appointment is confirmed. Your practice management system should prompt staff to verify all required fields, not just collect them.
Stage 2: Insurance Eligibility Verification
Eligibility verification is one of the most commonly skipped or rushed steps in medical billing, and one of the most costly when done carelessly.
Verifying eligibility once at the time of the first visit is not enough. Coverage changes. Patients switch jobs. Payers update their benefit structures. A policy that was active three weeks ago may have a different copay structure, a new deductible, or may have lapsed entirely.
Best-practice eligibility verification means:
- Checking eligibility in real time at every encounter, not just at first registration
- Confirming specific benefits relevant to the planned service (mental health coverage, specialist tiers, DME benefits)
- Verifying authorization requirements before the appointment, not after the visit
- Documenting verification results and saving them against the patient account
According to the AMS Solutions 2026 RCM Best Practices report, best-in-class practices verify insurance eligibility in real time at every patient encounter. This single discipline alone is one of the highest-leverage changes a billing team can make.
Stage 3: Prior Authorization
Prior authorization is now one of the leading drivers of claim denials across virtually every specialty. And the problem is getting worse, not better.
Prior authorization denials jumped 31% year over year in 2026, according to data from Qualigenix Healthcare. The CMS Interoperability and Prior Authorization Rule, which requires payers to respond faster and use standardized APIs, has changed the landscape, but only for providers who have adapted their workflows accordingly.
Practices that still rely on manual authorization tracking face a compounding problem: authorizations expire, services change, and staff forget to recheck. The result is a submitted claim that references an expired or incorrect authorization, which goes straight to denial.
A prevention-first approach to prior authorization includes:
- Using a centralized authorization log that tracks status, expiration dates, and service-specific requirements
- Assigning ownership to a specific team member for every open authorization
- Implementing automated alerts when an authorization is approaching its expiration date
- Checking authorization status within 48 hours of the scheduled service, not just at the time of the original request
At ProMantra, our prior authorization management process is built around exactly this kind of structured tracking. We work with providers across multiple specialties to maintain real-time authorization status visibility, which directly reduces the rate of authorization-related denials before claims are submitted.
Stage 4: Clinical Documentation and Coding Accuracy
Even if the first three stages are handled well, a coding error can undo all of it.
Coding-related denials are among the most preventable. They typically stem from one of a few recurring issues:
- Mismatched diagnosis and procedure codes (codes that don’t support medical necessity)
- Missing or incorrect modifiers
- Outdated codes following annual CPT and ICD-10 updates
- Upcoding or undercoding that triggers payer audits
The fix requires a dual commitment: keeping your coders current on annual code updates, and building a pre-submission review process into your workflow.
A clinical documentation improvement (CDI) program bridges the gap between what providers document in the clinical record and what coders need to assign the correct code. When providers and coders are aligned, claims go out cleaner, and payers have fewer grounds to deny them.
Building Your Prevention-First Billing Roadmap
Shifting from a reactive to a prevention-first model doesn’t happen overnight. But it doesn’t require a full-scale overhaul either. The following roadmap gives you a realistic path to start reducing preventable denials within the current billing cycle.
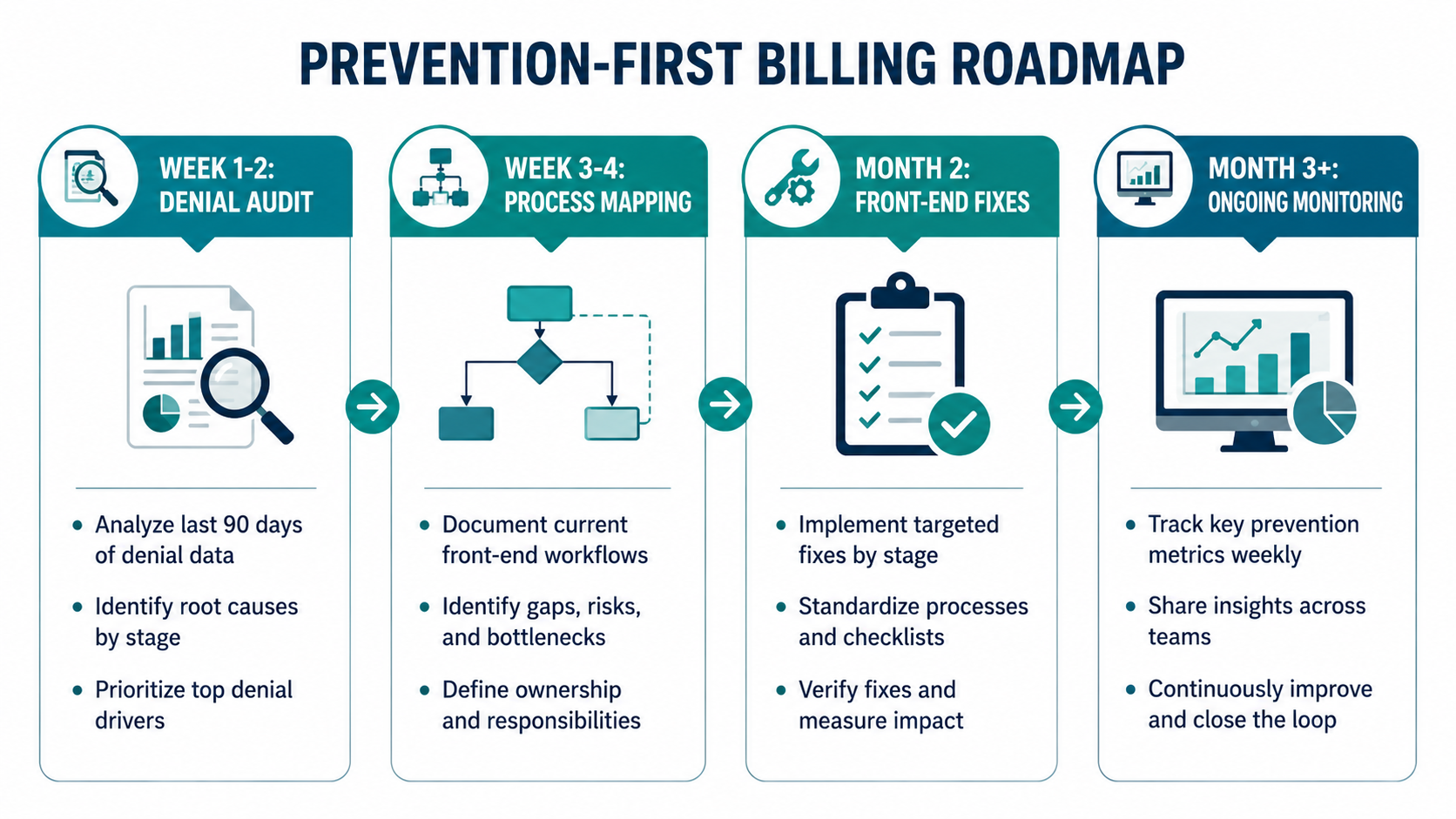
Step 1: Audit Your Current Denials by Root Cause
Before you fix anything, you need to know where your denials are actually coming from.
Pull the last 90 days of denial data and classify each denial by its root cause stage: registration, eligibility, authorization, or coding. Most practices find that a small number of recurring issue types account for the majority of their denial volume.
HFMA’s Revenue Cycle Improvement guidance notes that organizations with denial rates below 3% consistently track denial codes at a granular level and identify patterns by payer and by provider.
This audit gives you a priority list. You’re not fixing everything at once. You’re fixing the issues that are costing you the most first.
Step 2: Map Your Current Front-End Workflows
Take each of the four upstream stages and document what your team currently does. Be specific. How is eligibility verified? Who owns prior authorization tracking? What happens when a coder flags a documentation gap?
You’re looking for the cracks, the points where information is silently lost, assumptions are made, or steps are skipped under time pressure.
Step 3: Implement Targeted Fixes by Stage
Based on your audit and your workflow map, prioritize the front-end fixes that address your top denial drivers.
If authorization-related denials are your biggest problem, start with the authorization tracking system or explore how an automated denial tracking system can accelerate that process. If registration errors are frequent, start with your intake checklist. If coding accuracy is the issue, start with a CDI program and a claims scrubbing tool.
Pick one stage, build the fix, verify it’s working, and then move to the next. Trying to fix everything simultaneously rarely works and leads to incomplete implementation.
Step 4: Set Up Denial Prevention Metrics and Review Them Weekly
You can’t manage what you don’t measure. Define the metrics that tell you whether your prevention efforts are working:
- First-pass acceptance rate (target: 95% or higher)
- Authorization-related denial rate (target: under 2%)
- Eligibility-related denial rate (target: under 1%)
- Coding accuracy rate (target: 97% or higher)
- Overall initial denial rate (target: under 5%)
Review these in a weekly team huddle. Share them with clinical staff, not just billing staff. Denial prevention is not a billing department problem. It’s an organizational one.
Step 5: Close the Feedback Loop Between AR and Front-End Teams
This is the step most practices miss entirely.
When an AR specialist works a denial and discovers the root cause, that information needs to travel back to the team that originated the error, a principle at the heart of effective AR and front-end team alignment. If a coding mismatch caused a denial, the coder needs to know. If an eligibility gap caused it, the front-desk team needs to know.
Without a feedback loop, you fix individual denials but you never fix the process that keeps producing them.
What Prevention-First Billing Looks Like in Practice
Consider a multi-specialty practice that was seeing a denial rate of around 14%. After auditing their denial data, they discovered that over 40% of their denials were tied to authorization issues: expired auths, missing auths, and auths that didn’t cover the actual service rendered.
They implemented a centralized authorization tracker, assigned ownership by provider and service line, and added a 48-hour pre-service authorization check to every appointment workflow.
Within 90 days, their authorization-related denial rate dropped by more than half. Their overall denial rate fell to under 7%. Their AR team spent fewer hours on rework and more time on recovery of genuinely complex claims.
No new software was required. No staff were added. The gains came entirely from fixing the upstream process.
This is what denial prevention in medical billing actually delivers.
How ProMantra Supports a Prevention-First Revenue Cycle
At ProMantra, we’ve built our entire revenue cycle management approach around the principle that the best denial is the one that never happens.
Our team works with healthcare providers to audit existing denial patterns, identify the upstream gaps driving them, and implement the front-end workflows that close those gaps. From real-time eligibility verification and prior authorization tracking to coding accuracy reviews and claims scrubbing and real-time RCM automation, we handle the prevention side so your team can focus on patient care.
For practices that are already dealing with a high denial burden, we also provide denial recovery services that work the existing backlog while building the prevention infrastructure in parallel.
Frequently Asked Questions
- What is the difference between denial prevention and denial management in medical billing?
Denial management is reactive. It deals with claims that have already been denied, through appeals, resubmissions, and recovery. Denial prevention is proactive. It addresses the upstream process issues that cause denials before claims are ever submitted. Both are necessary, but prevention is significantly less expensive per claim and produces better long-term results.
- What are the most common causes of preventable claim denials?
The most common preventable denial causes fall into four categories: patient registration errors (incorrect demographics or insurance information), eligibility verification gaps (outdated or unverified coverage), prior authorization failures (missing, expired, or mismatched authorizations), and coding inaccuracies (mismatched diagnosis and procedure codes, missing modifiers, or use of outdated codes).
- How long does it take to see results from a prevention-first billing approach?
Most practices begin to see measurable improvement in their first-pass acceptance rate within 60 to 90 days of implementing targeted front-end fixes. The key is starting with a root-cause audit so you’re addressing the specific denial drivers in your practice rather than applying generic changes.
- Should small or independent practices invest in denial prevention processes?
Yes, and arguably more so than larger health systems. Small practices have less buffer to absorb write-offs and less staff capacity to manage high volumes of rework. A denial rate of even 8% can significantly affect a small practice’s cash flow. Prevention-first billing protects revenue and reduces the administrative burden on already-stretched billing staff.
Conclusion: Prevention Is the Strategy, Not Just a Best Practice
Treating denial prevention in medical billing as an afterthought costs your practice real money every single month. The data is clear, most denials are preventable, and the practices that keep denial rates below 5% have one thing in common: they intervene upstream, before claims leave the building.
The roadmap is not complicated. Audit your denials, map your workflows, fix the front-end gaps by stage, measure the right metrics, and close the feedback loop. Start with the stage causing the most damage and build from there.
Denials are not inevitable. They’re a symptom of fixable process problems.
Ready to stop reacting and start preventing?
Talk to ProMantra’s RCM team today and find out where your denial prevention gaps are, before they cost you another month of revenue.


