Every billing manager knows the feeling. A denial lands 45 days after the visit. The remark code points to something that went wrong in eligibility. Or authorization. Or registration. The claim was submitted correctly. The service was medically necessary. The coding was clean. But the damage was done weeks earlier, before the patient ever sat down in the exam room.
Front-end errors become back-end denials, sometimes 60 to 90 days later. By then, the patient is gone, the encounter is weeks old, and reconstructing the missing information takes more time than the original task would have.
According to MGMA, nearly 40% of claim denials originate from front-end errors, making early-stage optimization critical.
Yet most denial management strategies focus entirely on the back end. Teams spend hours drafting appeals, working AR queues, and chasing payers for claims that should never have been denied in the first place.
This blog identifies the five most common front-end gaps that silently generate back-end denials and gives you a specific, actionable fix for each one. By the time you finish reading, you will know exactly where to look and what to change.
Why Front-End Gaps Are So Damaging
The front end of your revenue cycle includes every workflow that happens before and during the patient encounter: scheduling, registration, insurance verification, prior authorization, and clinical documentation. These touchpoints set the foundation for every claim that follows.
When they go wrong, billing cannot fix it. Claims scrubbing tools can catch some mismatches. But they cannot recover a missing authorization or correct a demographic error that a payer’s adjudication engine has already flagged.
The 2025 State of Claims Report found that more than a quarter of respondents say that at least 10% of their denials result from inaccurate or incomplete data collected at patient intake, errors that occur during registration when critical patient information is first collected.
The average cost to rework a denied claim ranges from $25 to $118, depending on complexity. Multiply that across even 50 denied claims per week, and you are looking at a rework cost that compounds every billing cycle.
The fix is not to improve appeals. The fix is to stop producing the denials. Learn more about how to build a denial prevention system.
Gap 1: Registration Errors That Look Small but Cost Big
What Goes Wrong
Patient registration is the first data entry point in your revenue cycle. It is also the most error-prone, because it is high-volume, often rushed, and handled by staff with the highest turnover rates in the entire RCM department.
Missing or inaccurate patient data accounts for approximately 50% of denials. Common errors include incorrect name spelling, wrong date of birth, mismatched insurance ID, or outdated demographic information at intake.
A single transposed digit in a member ID. A name that does not match the insurance card because the patient recently married. A group number that was updated at renewal and never corrected in the system. Each of these looks trivial at the point of registration. Each of them becomes a denial 30 to 45 days later.
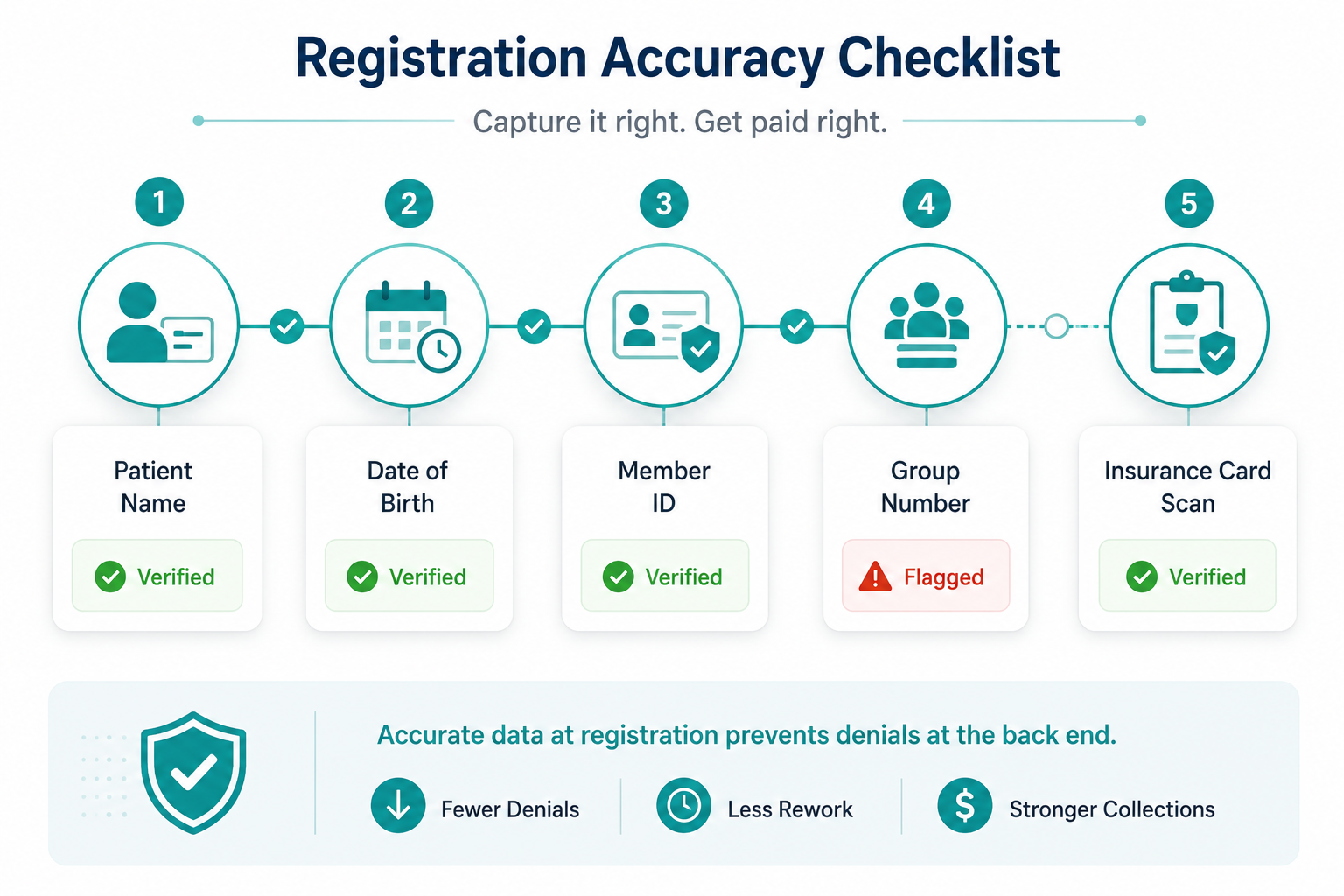
The Fix
- Implement a mandatory demographic verification step at every patient check-in, not just new patients. Existing patients change jobs, insurers, and names regularly.
- Use real-time eligibility (RTE) tools that validate patient information against payer databases at the point of scheduling, not the morning of the visit.
- Create a structured registration checklist that staff complete before closing each encounter. Include insurance card scan, photo ID verification, and member ID cross-check as required fields, not optional ones.
- Set up a monthly registration accuracy audit. Pull a sample of denied claims and trace how many originated from a registration field error. That number will tell you exactly how much this gap is costing you.
Gap 2: Eligibility Verification Done Once, Not Consistently
What Goes Wrong
Most practices check insurance eligibility. The problem is when they check it and how they use what they find.
Verifying eligibility once at the time of the first appointment is not sufficient. Coverage changes throughout the year. Patients switch employers, age off parents’ plans, enter and exit Medicaid eligibility windows, and change Medicare Advantage plans. A policy that was active at the last visit may have a new deductible, a different specialist tier, or may have lapsed entirely by the time of the next appointment.
Practices that verify eligibility at multiple touchpoints reduce denial rates by an estimated 20 to 30 percent compared to those that check only at registration. This single step has the highest return on effort in the entire revenue cycle.
When eligibility is checked once and filed away, the practice is billing based on stale data. Every encounter after that initial check is a potential denial waiting to be triggered.
The Fix
- Verify eligibility at three points: at scheduling, 24 to 48 hours before the appointment, and again at check-in for high-cost or high-risk procedures.
- Document the verification result against each encounter, not just in the patient record. This creates a defensible trail if a payer disputes eligibility at the time of adjudication.
- For high-volume specialties, automate eligibility checks via your practice management system so the verification runs on a scheduled basis without manual intervention.
- Flag patients whose coverage has changed since their last visit and route them for financial counseling before the service is rendered, not after the claim is denied.
Gap 3: Prior Authorization Gaps That Slip Through Workflow Cracks
What Goes Wrong
Prior authorization is consistently ranked among the top three denial drivers across every major survey of revenue cycle leaders.
Prior authorization issues continue to rank as a top operational challenge that triggers claim denials, with 35% of survey respondents identifying authorizations as a primary trigger according to Experian Health’s State of Claims 2025 report.
The failure is rarely that staff do not know authorization is required. The failure is in the workflow gaps around tracking it. An authorization is obtained but the number is entered incorrectly on the claim. An authorization is approved for a service but the actual service rendered differs slightly from what was authorized. An authorization is valid at the time of scheduling but expires before the service date. A provider sees a patient urgently and the service is rendered before authorization is confirmed.
Prior authorization errors, including missing authorization, expired authorization, or failure to document the authorization number correctly on the claim, account for approximately 35% of denials.
Each of these is a workflow failure, not a knowledge failure. The team knew authorization was needed. The process did not catch the gap.
The Fix
- Build a centralized authorization tracking log that records the authorization number, service authorized, expiration date, and the specific CPT codes covered. Review it 48 hours before every scheduled service.
- Assign ownership. Every open authorization should have a named staff member responsible for monitoring its status and expiration. Shared responsibility means no one is accountable.
- When an authorization is obtained, cross-reference the approved service against the planned service at the time of scheduling confirmation, not the day of the visit.
- Create a pre-service authorization check as a required step in your appointment confirmation workflow for any service that carries an authorization requirement.
Gap 4: Clinical Documentation That Does Not Support the Claim
What Goes Wrong
Payers are using increasingly sophisticated tools to cross-reference what was billed against what was documented. A claim that shows a Level 4 E/M visit billed but a clinical note that documents a straightforward complaint and a brief exam will be flagged for medical necessity review or downcoded.
According to AKASA’s survey of more than 350 CFOs and financial leaders at US health systems, lack of documentation to support medical necessity and physician documentation issues are among the top five reasons for initial payer denials.
The problem is structural. Physicians document for clinical purposes, not billing purposes. They capture what is clinically relevant to the patient encounter. They do not always capture what a payer needs to see to justify the level of service billed.
This is not a physician error. It is a systems and education gap between clinical documentation and revenue cycle requirements.
The Fix
- Implement a clinical documentation improvement (CDI) program that provides providers with specialty-specific documentation templates tied to the CPT codes most commonly billed in your practice.
- Create a feedback loop between denied claims and the clinical team. When a claim is denied for insufficient documentation, that information should reach the provider, not sit in the billing department.
- Run monthly concurrent coding audits where a sample of recent encounters is reviewed for documentation-to-code alignment while the encounter is still relatively fresh. Catching the gap 30 days out is far better than catching it after a denial.
- For high-risk CPT codes, build a pre-submission documentation check into your workflow that flags encounters where the clinical note does not meet the minimum documentation threshold for the billed level of service.
Gap 5: Credentialing Lapses Nobody Notices Until the Denials Pile Up
What Goes Wrong
This is the front-end gap that most practices discover the hardest way.
When a provider’s credentials expire with a payer, or when a new provider is seeing patients before their enrollment is fully complete, every claim submitted under that provider can be denied. Retroactively. Not just going forward, but for every claim that was submitted during the gap period.
When a provider’s credentials expire or their payer enrollment lapses, payers can deny claims retroactively, not just going forward. In a high-volume practice, even a two-week credentialing gap can generate hundreds of thousands of dollars in denied claims.
Credentialing is often managed as a one-time task. A provider joins the practice, credentialing is completed, and the file is closed. But payer enrollments have expiration dates. Re-credentialing cycles vary by payer. Medicare and Medicaid have revalidation requirements with specific timelines. Private payers have their own renewal windows.
Without a system to track all of this, a lapse happens quietly. The claims go out. The denials come back. And by then, the gap may already be weeks old.
The Fix
- Build a credentialing expiration calendar that tracks every provider’s enrollment status with every active payer, including revalidation dates, re-credentialing cycles, and Medicare/Medicaid revalidation windows.
- Set automated alerts at 90 days, 60 days, and 30 days before any credential expiration. Do not rely on manual calendar reminders.
- When a new provider joins the practice, establish a clear policy that limits the services they can bill under until their credentialing is fully confirmed. Billing under a supervising provider’s credentials is permissible in some situations but must be done correctly and documented accordingly.
- Conduct a credentialing audit at least twice per year. Pull your active provider list and verify current enrollment status with your five highest-volume payers for each provider.
The Denial Fingerprint: Tracing Every Back-End Denial to Its Front-End Source
Most billing teams categorize denials by the code that comes back from the payer. CO-197 means authorization. CO-16 means missing information. CO-50 means medical necessity.
But the code tells you what the payer rejected, not where in your workflow the problem was created.
A denial prevention strategy requires mapping each denial code back to the specific front-end stage where the gap occurred. Authorization denials trace to Gap 3. Medical necessity denials trace to Gap 4. Demographic mismatches trace to Gap 1. Eligibility denials trace to Gap 2. Credentialing denials trace to Gap 5.
When you build this map for your own practice using 90 days of denial data, you will almost always find that a small number of front-end process failures are responsible for the majority of your denial volume.
Fix those process failures, and the denials that depend on them disappear.
How ProMantra Closes These Gaps for Healthcare Providers
At ProMantra, we work with healthcare providers across multiple specialties to build the front-end workflows that stop these five gaps from generating back-end denials.
Our team conducts structured denial root-cause audits that trace denial patterns by code, payer, provider, and service line back to their upstream origin. We identify which of the five gaps is producing the most denial volume for your specific practice, build the workflows to close them, and create a monitoring system to catch new gaps before they compound.
For practices dealing with a high existing denial burden, we also handle denial recovery in parallel while building the prevention infrastructure, so you are not waiting months to see financial improvement.
If your billing team is spending its days working denials instead of preventing them, the conversation starts with finding out where your denials are actually being born.
Frequently Asked Questions
- What percentage of claim denials actually originate from front-end errors?
Research consistently points to front-end errors as the primary driver of claim denials. MGMA data indicates that nearly 40% of claim denials originate from front-end errors. Experian Health’s State of Claims 2025 report found that more than a quarter of providers say at least 10% of their denials result from inaccurate or incomplete data collected at patient intake alone. When authorization failures and documentation gaps are included, the front-end share of total denial volume is substantially higher.
- How often should a practice verify insurance eligibility?
Best practice is to verify eligibility at a minimum of three points: at the time of scheduling, 24 to 48 hours before the appointment, and again at check-in for high-cost or specialty procedures. Practices that verify eligibility at multiple touchpoints see estimated denial rate reductions of 20 to 30 percent compared to those that check only once at initial registration.
- What is a denial fingerprint and how does it help prevent denials?
A denial fingerprint is the process of mapping each denial type back to the specific front-end workflow stage where the error originated, rather than simply categorizing it by the payer’s remark code. For example, a CO-197 authorization denial traces back to a gap in your prior authorization tracking workflow. A CO-16 missing information denial traces back to a registration or documentation gap. This mapping gives billing leaders a prioritized list of front-end process fixes based on actual denial impact rather than general best practices.
- How do credentialing lapses cause claim denials and how quickly can they be discovered?
When a provider’s payer enrollment or credential expires, payers can deny claims submitted under that provider retroactively for the entire period of the lapse. In a high-volume practice, even a two-week gap can generate significant denial volume. The challenge is that these denials often do not surface until 30 to 60 days after the claims are submitted, by which point the lapse may be weeks old. A proactive credentialing calendar with expiration alerts at 90, 60, and 30 days prevents the gap from occurring in the first place.
Conclusion: The Denial Starts Before the Claim Does
Back-end denial management will always be part of revenue cycle operations. Payers will always push back on some percentage of claims. But the majority of denial volume most practices deal with every day is preventable.
The five gaps described in this blog are registration errors, inconsistent eligibility verification, prior authorization workflow cracks, clinical documentation misalignment, and credentialing lapses. None of them are new problems. All of them are fixable with the right workflow design and the right accountability structure.
The practices that keep denial rates below 5% do not have better billers than everyone else. They have better front-end processes that stop producing the errors that generate denials in the first place.
Start with your last 90 days of denial data. Classify every denial by its root-cause stage using the five-gap framework above. The gaps that are costing you the most will become immediately clear, and so will the fixes that will have the highest impact on your revenue.
Ready to find out which of these five gaps is driving the most denials in your practice?
ProMantra offers a structured denial root-cause audit that traces your denial patterns back to their front-end source and identifies the specific workflow fixes that will move your numbers. Contact our team today to get started.