If your health system is running, or planning to launch, a hospital-at-home program, your revenue cycle team is facing a billing environment that looks nothing like traditional inpatient care. Claims for hospital-at-home programs still move through the Medicare inpatient framework, but the documentation, coding, and payer rules around them are new enough that most billing teams are still catching up. Add in a five-year federal waiver extension that just turned a pilot-stage model into a long-term care setting, and revenue cycle leaders now have a narrow window to get the fundamentals right before volume outpaces process.
This article walks through what changed in 2026, where the revenue cycle risk actually sits, and what a well-built strategy looks like for protecting reimbursement as hospital-at-home programs scale into a permanent part of the inpatient mix.
What Are Hospital-at-Home Programs, and Why Are They Growing So Fast?
Hospital-at-home programs let approved hospitals deliver inpatient-level acute care to patients in their own homes instead of a hospital bed. The model runs under the Acute Hospital Care at Home (AHCAH) waiver, which suspends specific hospital Conditions of Participation, most notably the requirement for 24/7 on-premises nursing, so qualifying patients can receive hospital-grade monitoring, medication, and physician oversight without leaving home.
The program has moved well past pilot status. In early 2026, Congress passed a five-year extension of the AHCAH waiver through September 30, 2030, giving hospitals the regulatory certainty to invest in hospital-at-home infrastructure rather than treat it as a temporary experiment tied to short-term funding bills. Hundreds of programs across dozens of states are now approved, and more health systems are actively building capacity in response to strong patient demand for care delivered outside a traditional hospital room. For a broader look at how these dynamics fit into overall inpatient financial performance, our hospital revenue cycle management guide covers the fundamentals every finance leader should already have in place before layering a hospital-at-home program on top.
How Hospital-at-Home Claims Actually Get Billed
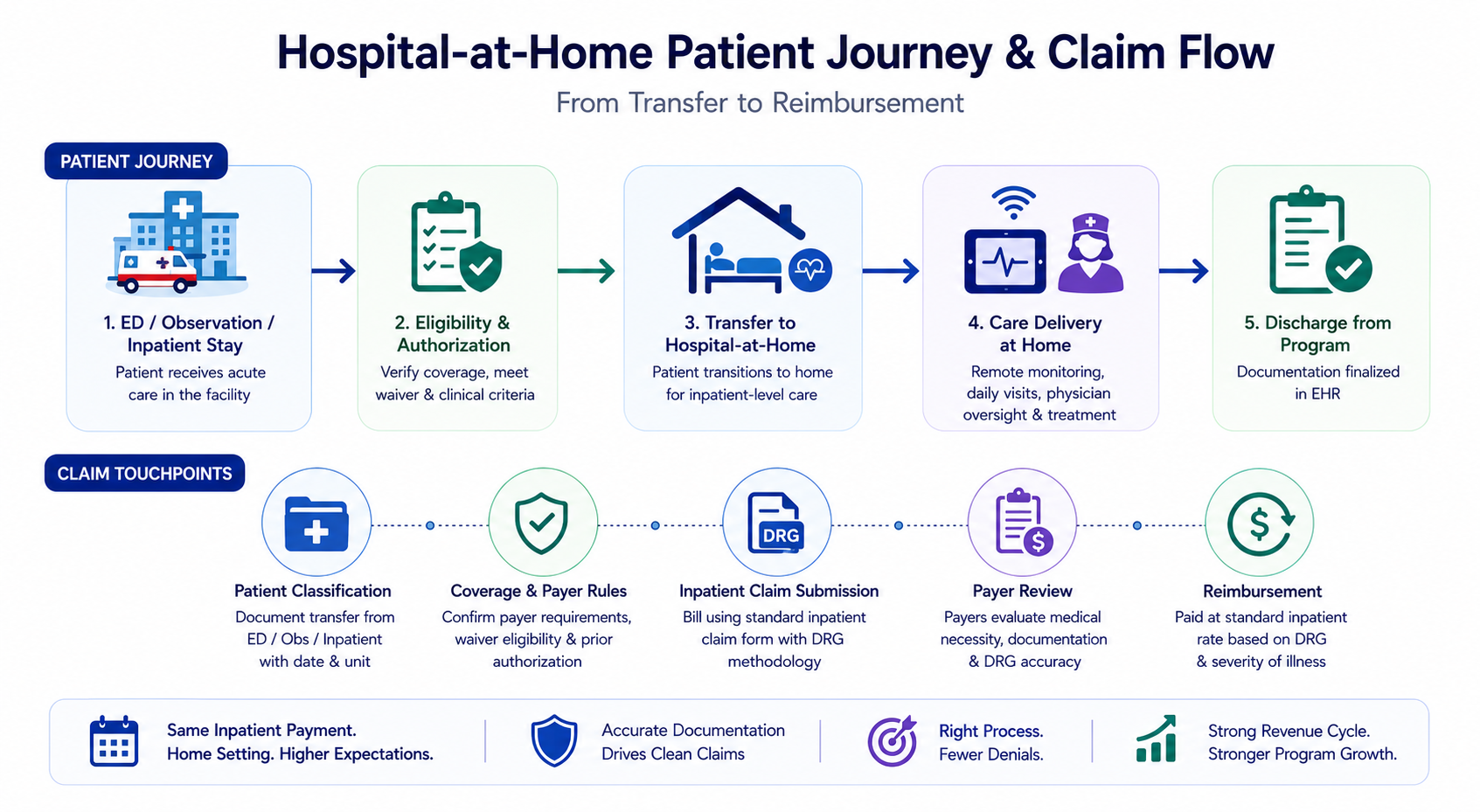
Unlike home health or routine remote patient monitoring, hospital-at-home programs bill as acute inpatient care. That single distinction drives almost every revenue cycle decision that follows, from documentation standards to denial management priorities.
Hospitals submit hospital-at-home claims using the same inpatient claim form and diagnosis-related group methodology used for a traditional hospital stay. There is no separate payment for delivering care in the home; the hospital is reimbursed at the standard inpatient rate based on the patient’s diagnosis and clinical complexity. Because the care happens at a home address, claims must also clearly show that the patient was transferred from an emergency department, observation status, or an existing inpatient stay into the program, with the transfer date and originating unit documented consistently. Getting that classification right depends on billing expertise that already understands acute inpatient nuance, which is exactly where our hospitalist billing services team spends most of its time today.
Payer variability adds another layer many programs underestimate early on. Traditional Medicare follows the federal waiver rules directly, but Medicare Advantage plans and commercial payers each set their own coverage terms, authorization requirements, and documentation expectations, and these can change from one plan year to the next. A process built only around Medicare rules will run into denials the moment a Medicare Advantage or commercial claim hits different payer edits, so hospital-at-home programs need a revenue cycle management strategy that flexes across payer types.
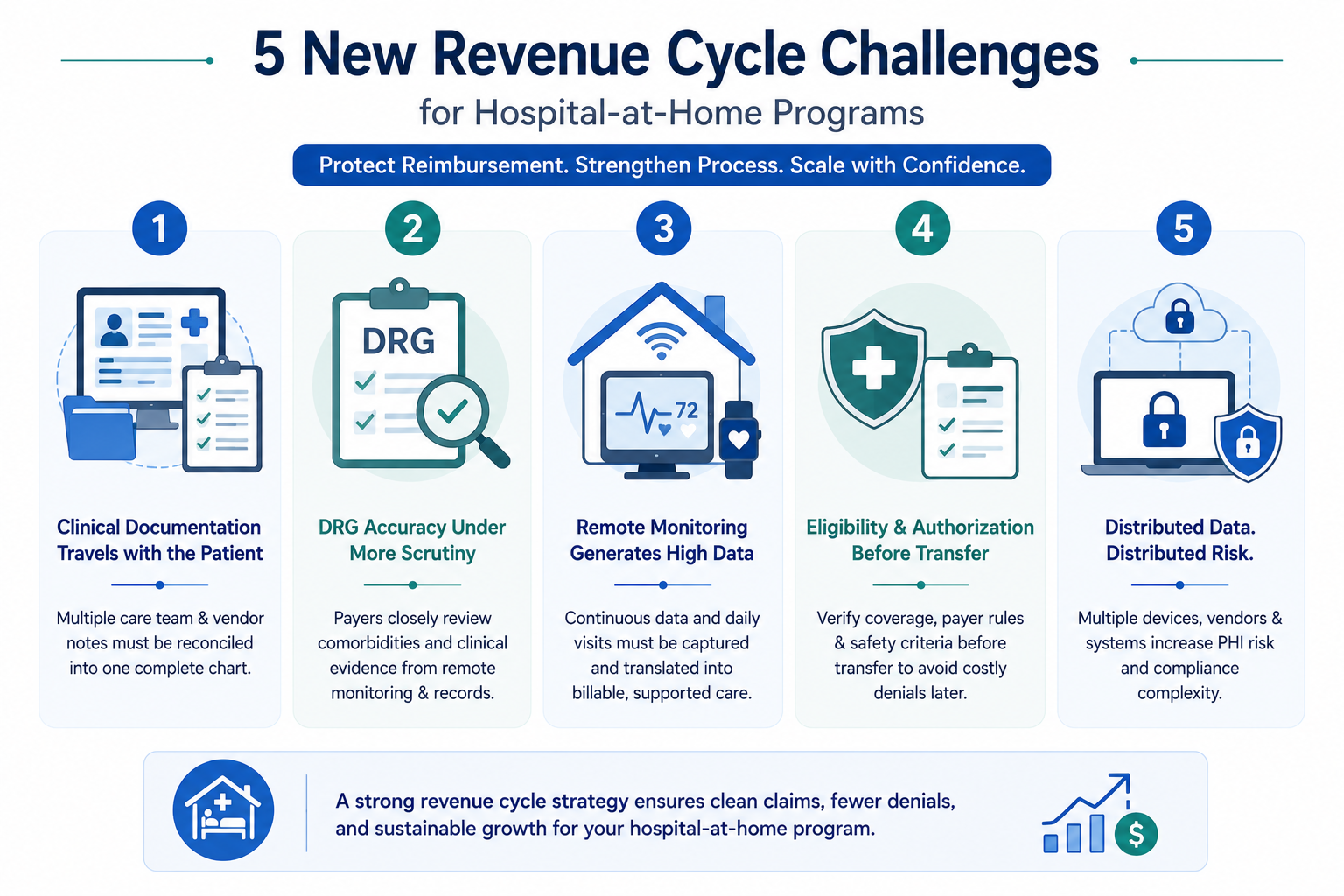
Five New Revenue Cycle Challenges Hospital-at-Home Programs Must Solve
- Clinical documentation has to travel with the patient. In a traditional inpatient stay, physicians, nurses, and coders work under one roof with shared systems. In a hospital-at-home model, care teams, remote monitoring vendors, and in-home visiting staff all generate documentation separately, and it has to be reconciled into one coherent chart before a clean claim can go out. A recent look at medical necessity documentation gaps found that missing or inconsistent notes remain a leading cause of preventable denials across acute care settings, and this risk is amplified because documentation sources are physically scattered across vendors and locations.
- Diagnosis-related group accuracy is under more scrutiny than ever. Since hospital-at-home stays bill through the same diagnosis-related group system as traditional admissions, they are just as exposed to clinical validation denials, and arguably more so. Payers increasingly challenge cases where a comorbidity is coded but not clearly supported by treatment notes, vitals, or medication records pulled from remote monitoring systems that coders may not routinely review. Hospital-at-home programs need coders who understand both diagnosis-related group logic and remote care documentation, which is exactly the kind of mismatch our RevvPro platform is built to flag before a claim leaves the building.
- Remote monitoring generates data volume that charge capture was not built for. Continuous vitals tracking, medication reminders, video check-ins, and the two required daily in-person visits all generate a steady stream of clinical activity. Without a workflow that translates that activity into billable, well-documented services, hospitals leave utilization evidence on the table that could otherwise support a stronger DRG assignment. Our earlier piece on telehealth billing trends covers a similar challenge, where remote care documentation carries stakes just as high as an in-person encounter.
- Eligibility and authorization checks need to happen before transfer, not after. A patient typically moves into a hospital-at-home program directly from an emergency department, observation unit, or existing inpatient bed. That transfer point is also when eligibility, payer-specific authorization, and safety criteria need to be confirmed. Because these decisions happen quickly, front-end verification teams often skip steps that would normally slow down a traditional admission, and those steps tend to surface weeks later as denials. Strong healthcare IT solutions that connect eligibility verification directly to the discharge and transfer workflow help close that gap before it becomes a claim problem.
- Distributed care means distributed data, and distributed risk. Vitals monitors, video platforms, in-home tablets, and connected EHR systems all touch protected health information outside the traditional hospital perimeter. A recent look at data security in outsourced RCM environments highlights how CFOs are increasingly asked to verify security controls across every vendor touching patient data, and hospital-at-home programs multiply the number of endpoints a compliance team must track.
Building a Revenue Cycle Strategy That Keeps Pace With Growth
Getting hospital-at-home billing right is less about a single fix and more about aligning three things consistently: documentation workflow, coding expertise, and technology that can follow a patient outside hospital walls without losing visibility along the way.
The strongest hospital-at-home programs build documentation checkpoints directly into the daily nursing and physician visit schedule, instead of trying to reconstruct a clean record during coding after the patient has already been discharged from the program. This proactive habit also supports the kind of quality and outcomes reporting increasingly tied to reimbursement, an area covered in our recent piece on value-based payment models, since these programs sit squarely at the intersection of clinical outcomes and financial performance.
Diagnosis-related group coding for hospital-at-home patients requires the same rigor as any inpatient stay, plus real familiarity with how remote monitoring data supports or challenges a given code assignment. Ongoing training, not a one-time policy update, is what keeps clean claim rates high as payer scrutiny of these claims continues to increase year over year. Because this data lives across so many separate systems, a strong health information management framework that consolidates records, tracks access, and supports HIPAA-aligned data handling is no longer optional. It is the backbone that keeps a fast-growing hospital-at-home program audit-ready as claim volume climbs.
How ProMantra Supports Hospital-at-Home Revenue Cycle Performance
ProMantra has spent more than two decades helping hospitals, health systems, and specialty practices strengthen their revenue cycle operations, and hospital-at-home programs bring exactly the kind of documentation and coding complexity our team is built for. We are HIPAA compliant and ISO 27001 certified, which matters directly for programs handling patient data across distributed home-based care environments. Our coders, denial management specialists, and account managers work alongside these care teams to close documentation gaps, keep diagnosis-related group coding accurate, and verify eligibility and authorization before a patient ever transfers into the program. As program volume grows through 2030, having a revenue cycle partner who understands both traditional inpatient billing and the operational realities of remote care can be the difference between a program that scales profitably and one that quietly loses revenue along the way.
Frequently Asked Questions
- Do hospital-at-home programs get reimbursed differently than a regular hospital stay? No. Hospital-at-home claims are billed and reimbursed through the same inpatient diagnosis-related group methodology as a traditional hospital admission. There is no separate home-care payment; the hospital receives the standard inpatient rate for the patient’s diagnosis and clinical complexity.
- What is the biggest revenue cycle risk in hospital-at-home billing? Documentation fragmentation is the most common risk. Because clinical notes come from remote monitoring vendors, visiting nurses, and physicians working outside a single hospital system, reconciling that documentation into a clean, defensible claim is harder than in a traditional inpatient stay.
- How long is the CMS hospital-at-home waiver extended? Congress extended the Acute Hospital Care at Home waiver for five years, through September 30, 2030, giving hospitals long-term regulatory certainty to invest in program infrastructure.
- Do Medicare Advantage and commercial payers follow the same hospital-at-home billing rules as traditional Medicare? Not always. While traditional Medicare follows the federal waiver rules directly, Medicare Advantage plans and commercial payers can set their own authorization requirements and documentation expectations, which is why payer-specific verification matters.
- How can hospitals reduce denials in a growing hospital-at-home program? Reducing denials generally comes down to three things: aligning clinical documentation at the point of care, using coders trained in both inpatient and remote care nuances, and verifying eligibility and authorization before the patient transfers into the program rather than after.
Ready to strengthen the revenue cycle behind your hospital-at-home program? Contact ProMantra for a free RCM assessment tailored to hospital-at-home and inpatient billing.